Golf and Skin Health: A Narrative Review
Article information

Abstract
OBJECTIVES
Recent studies have reported that playing golf has overall physical and mental health benefits. Through being placed in the sun for extended periods of time, the golfing population faces an increased risk of ultraviolet radiation (UVR) associated skin problems, most importantly skin cancer. Our aim was to collate and summarise current literature on the relationship between golf and skin cancer.
METHODS
We searched multiple web-based, health-focused databases (Medline, Embase, Cinahl, Web of science, Scopus, Sportdiscus, UK clinical trials, Current controlled trials and Prospero) to identify records. Relevant papers were critically appraised and reported using a descriptive analysis.
RESULTS
A total of 11 studies are included in the review. Golf is associated with relatively more UVR exposure than other outdoor activities such as fishing, tennis, pool swimming, cricket, gardening, ‘sun-worshipping’ and sailing. Calculated relative risk of non- melanoma skin cancer, based on cumulative UV exposure, is higher in golfers than non-golfers. Mid morning tee-times or playing golf between 11am -3pm associated with highest UVR exposures. Golfers can be exposed to potentially harmful levels of UVR during play in winter at some latitudes. Vertex (scalp), shoulders, back, back of neck and posterior arms exposed to more UVR than front of body during play. Common golf attire is of limited value in protecting the neck. Targeted skin cancer skin cancer prevention and early detection campaigns are well received among the golfing population.
CONCLUSIONS
Overall, playing golf is associated with longevity and both physical and mental health benefits. Studies to date indicate that golfers (professionals > recreational players) are exposed to potentially harmful levels of UVR during play, but the true morbidity/mortality associated with this exposure is not known. Playing golf should be encouraged in all age groups, though golfers, the golf industry and policy makers should act to minimize the harmful effects of UVR exposure, and have they have ability to also be hugely influential on an important public health message.
INTRODUCTION
Exposure to ultraviolet radiation (UVR) is the most important environmental risk factor in the development of cutaneous melanoma and non-melanoma skin cancers (basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)), rates of which have been steadily increasing worldwide over the last 40 years [1]. UVR can also cause painful sunburn reactions, skin pigment changes, accelerated skin ageing and eye disorders such as cataracts. Conversely, UVR has important health benefits. Exposure to ultraviolet-B (UVB) radiation stimulates vitamin-D production, which is essential for skeletal health and optimal immune function [2]. There is emerging evidence that UVR has beneficial effects on cardiovascular risk factors independently of Vitamin D [3]. Sunlight is also known to have mood-lifting effects [4].
Playing golf has overall physical and mental health benefits, [5,6] however by being placed in the sun for extended periods of time, the golfing population face an increased risk of UVR associated skin problems, most importantly skin cancer. Literature pertaining specifically to skin problems encountered by the golfing population is varied in its focus and quality. The aim of this narrative review was to collate and summarise this literature.
MATERIALS AND METHODS
Search Strategy
The following health focused databases and search platforms were used to search for studies: Medline, Embase, Cinahl, Web of science, Scopus, Sportdiscus, UK clinical trials, Current controlled trials and Prospero.
Eligibility criteria
The following inclusion and exclusion criteria were utilized:
a. Inclusion criteria
• English language articles only
• All age groups and both sexes of participants
• Research undertaken in both professional and recreational golfers and golf spectators
• Research articles discussing any aspect of skin health and/or ultraviolet radiation exposure in context of golf
• Sources of information can include primary research studies, reviews (including but not limited to systematic reviews, scoping reviews, meta-analyses), guidelines, as well as grey literature to include unpublished and on-going trials, annual reports, dissertations, and conference proceedings.
• Research articles not limited by geographical location, language, research setting or date of research
b. Explicit exclusion criteria
• Opinion pieces/ opinions, magazine and newspaper articles, case reports, papers with no data.
Search Terms
Each database was searched using the primary search term “golf ”. From this secondary search terms: “skin”, “skin health”, “skin cancer”, “skin neoplasm”, “melanoma”, “basal cell carcinoma”, “squamous cell carcinoma”, “ultraviolet radiation”, “sun”, “sunlight”, “photoaging”, “Vitamin D” were used to narrow down eligible papers relating to golf and skin health. Two reviewers (AGM and HP) assessed the titles and abstracts applying the eligibility criteria. The same two reviewers appraised the selected papers. Additional studies were identified from the reference lists of included papers.
Analysis
A descriptive analysis was used to summarise the evidence collected.
RESULTS
The initial data search using the term ‘golf ’ yielded a total of 1871 records. Review using the secondary terms of titles and/or abstracts excluded 1816 records, leaving 55 records to be assessed against our eligibility criteria. Critical appraisal of these records and review of their references identified a total of 11 studies relevant to our review that focused on golf and skin health (PRISMA flow diagram) (Figure 1).

Prisma flow diagram
Method of study
The majority of studies relating to golf and skin health focus on UVR dosimetry as their method of data collection [7-13]. Population- We identified one study that reports on skin cancer prevalence in female golfers, with the rest focusing on a male population [14].
Sun protection practice
There are two studies examining sun-protection practices in golfers/golf spectators [15,16] highlighting that sun protection practice is generally poor, however education such as demonstrating current skin photo-damage has the ability to increase intention of taking up protective measures [12]. One study evaluates the feasibility and effectiveness of a targeted skin cancer prevention and an early detection campaign in golfers and golf-course workers [17], and also highlighted that a significant number of participants (99.3%) after planned to improve their habits to sun exposure after this awareness was introduced. The back of the neck and wrist were found to have the highest UVR exposure [11,13]. Clothing is an important and easy tool in reducing UVR transmission, however common golfing attire is limited in protecting the back of the neck [10].
UVR exposure
Papers that studied outdoor activities found that golf is associated with higher UVR exposure than other outdoor activities such as tennis, sailing and fishing which many people are aware of as a high UVR exposure activity, however the study also demonstrated that environmental and behaviour will determine overall exposure [7,8]. Golfing attire is not routinely tested for UVR transmittance. Professionals are exposed to higher UVR levels than amateurs, predominantly due to time on golf course, playing year-round and travelling to follow an temperate climate for practice and tournaments, therefore increasing overall high level UVR exposure. The key findings for each study are summarised in Table 1.

Key Findings
DISCUSSION
Golfers (both professional, amateur and caddies) can be exposed to potentially harmful levels of UVR during play and outdoor practice [7-14]. Golf is played all over the world, and the level of UVR to which an individual golfer’s skin is exposed during play is dependent on a number of situational and personal variables including location of play (latitude & altitude), season, tee time, duration of play, cloud cover, other weather conditions, facility factors (level of natural shade etc) and protective behavior (clothing choice and use of sunscreen) [18]. The use of sun protection practice seems to be poor, highlighting a key area for possible intervention. Cumulative UVR exposure - the key risk factor for development of primary cutaneous SCC - over a golfing-lifetime is dependent on frequency of play in conditions conducive to high UVR exposure, hence the increased risk for professional golfers who travel to temperate climate golf locations over the world and therefore increase their UVR exposure. The association between excessive UVR exposure and skin cancer is well documented, but the level of harm caused by UVR to the skin of a golfer is not only influenced by dose absorbed, but also skin type, number of melanonaevi, medical history and family history [19]. ‘Outdoor workers’, professional golfers, caddies and green keepers undoubtedly carry an increased risk of skin cancer through high UVR exposures [20,21], though this has not been proven with large-scale epidemiological studies in these specific groups. Recreational players probably have an overall lower risk than professionals. Golf can therefore pose an individual at risk, highlighting a key area for public health targeting and awareness needed. It has been seen from the qualitative studies that many golfers have little awareness on their risk of harmful UVR exposure, and simple educational awareness raising measures can have the potential to have a large public health impact on skin health.
There are currently no studies examining the morbidity and mortality associated with skin cancer in a golfing population, however overall, playing golf is associated with longevity, and physical health benefits [5]. The best understood beneficial effect of UVR is the synthesis of vitamin-D. Vitamin-D production requires exposure to UVB radiation, which causes sunburn and is more carcinogenic than UVA. It has been consistently shown that vitamin D can be efficiently and sufficiently produced at doses of UVB below those which cause sunburn in most people; and that prolonged exposure provides no additional vitamin D but linearly increases levels of DNA damage and risk of skin cancer. Thus, over-exposure to UVR resulting in sunburn and heavy tanning cannot be justified [22]. There is emerging evidence that sunshine has major health benefits independent of Vitamin-D but the mechanisms and impact require further research [3,23].
In summary, playing golf should be encouraged in all age groups due to overall health and well-being benefits, while golfers, the golf industry and policy makers should act to minimise harmful effects of UV radiation. As golf is played worldwide and in all seasons by a whole mix of skin types, potential harm from UV radiation will vary from player to player. The studies examined in this paper, in addition to the general literature on sun protection [24] support the key ‘golf orientated’ health promotion messages outlined in Table 2.
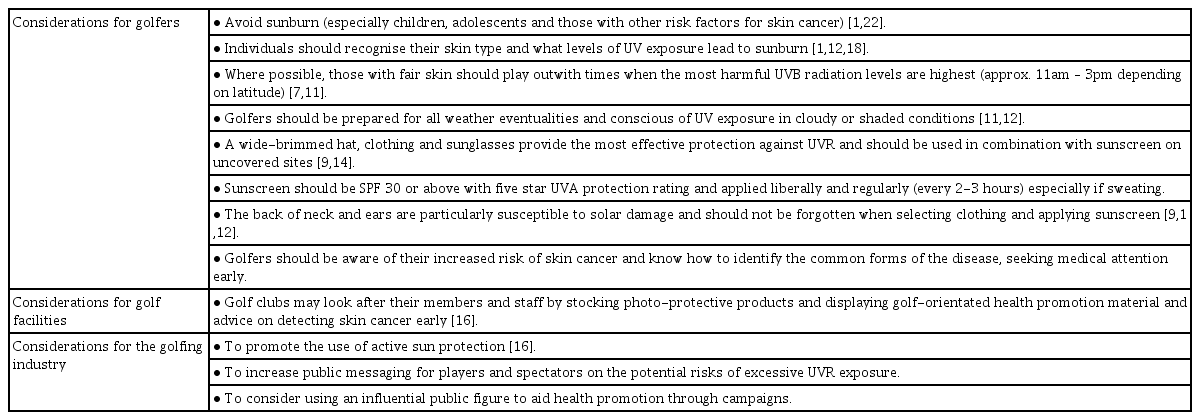
Considerations
Active sun protection will always be dependent on attitudes and subsequent behaviors, which can vary widely. Therefore, in addition to striving to be as safe as possible in the sunshine, golfers should also be aware of their risk of skin cancer and know how to identify the common forms of the disease, seeking medical attention early. In view of their high level of occupational UVR exposure, professional golfers, caddies and golf industry workers are likely to benefit from targeted health promotion and skin cancer screening. This is an area that the golfing industry would be able to have a significant positive impact on through education, awareness and publication.
CONCLUSIONS
Overall, playing golf is associated with longevity, and both physical and mental health benefits. However, by being placed in the sun for extended periods of time, the golfing population faces an increased risk of UVR associated skin problems, most importantly skin cancer. Studies to date indicate that golfers are definitely exposed to potentially harmful levels of UVR during play and outdoor practice, but the morbidity/mortality related to this exposure is not known. More large-scale epidemiological studies are required to determine the true risk to skin health from playing golf (both professionally and recreationally) and the effectiveness of active sun protection and targeted health promotion at modifying outcomes in this group. Meantime, golfers are encouraged to take the sensible steps outlined in this paper to reduce their level of UV exposure during play. Golf facilities and the golf industry should take an active role in supporting golfers to reduce their level of UV exposure and empower them to be able to detect skin cancer early.
Notes
Conflict of Interest
The authors declare no conflict of interest.