


INTRODUCTION
Self-regulation is defined as the “monitoring and management of the self, by the self, so that behavior can be appropriately controlled” [1]. Behavioral self-regulation, social skills, and the ability to maintain focus and attention are important skills that impact school readiness [2,3]. Self-regulation must develop rapidly during early childhood [4], as it is fundamental to successful participation in preschool and kindergarten settings [5-7]. Since self-regulation skills are strongly associated with social functioning [8-10], children lacking self-regulation skills are often unable to attend school with peers or participate in group activities. Parents of children lacking self-regulation skills report “avoidance of public spaces and programs” because of their children’s disruptive behaviors, extreme separation anxiety, or fear/difficulty with transitions (CL and JC, personal communication).
Little is known about self-regulation in children with developmental delays. Hypothetically, children with communication, self-regulation or behavioral issues would be expected to have difficulty adjusting to the demands of a classroom or group setting. Young children who experience such limitations typically lack the skills needed to benefit from or even participate in therapy interventions [11]. The explicit teaching of communication and self-regulation skills is required in order for these children to be able to learn [12]. A combined approach to enhancing both communication and self-regulation skills is thought to be an appropriate intervention strategy [13], but standardized programs that combine these two types of therapy have not been developed or evaluated.
Physically active play is a pre-requisite for normal childhood development, childhood socialization and strong parent-child bonds [14,15]. Tumbling TogetherTM is an intensive program offered by a specialized, inter-professional team through the medium of a kinder-gym gymnastics class [16]. Its purpose is to develop self-regulation skills in children 3 to 5 years of age with significant developmental, behavioral, or social delays (e.g., autism spectrum disorder, language/communication disorder, developmental delay, anxiety). Children attending Tumbling TogetherTM are referred to the program by a healthcare professional and must have previously demonstrated an inability to understand, cope with or adhere to group activities or expectations.
The characteristics of limited self-regulation, such as the inability to maintain focus or respond appropriately to environmental change, limit the effectiveness of standard evaluation techniques (e.g., an objective examiner or standardized assessment protocol). The goal of this study was to determine whether video recordings of the program participants could be used to objectively evaluate the self-regulation skills of preschool-aged children. Specifically, we wondered whether video-recordings could be used to document the children’s: a) response to a command, b) response to an action signal, and c) ability to wait for a turn. We also sought to evaluate whether the video recording would disrupt delivery of the program due to the children’s inability to maintain focus.
METHODS
Study Design
Our prospective, pre/post study design evaluated the feasibility of video recording to assess self-regulation among children attending the Tumbling TogetherTM exercise intervention. The intervention was delivered to small groups of children (maximum of 8 children per group) by the interdisciplinary team of Tumbling TogetherTM rehabilitation professionals and volunteers. Each group of children attended one 45-minute session per week for either 8 (2 groups) or 10 (2 groups) weeks. Baseline assessments (first and second week) evaluated self-regulation before program instruction. Post-program assessments (second-last and last week) were completed during the last two sessions for each cohort.
Written parental consent for each child’s study participation was obtained prior to or on arrival for the first session. Ethics approvals for the study were obtained from the Children’s Hospital of Eastern Ontario Research Ethics Board (IRB#13/146X), as well as the Brockville General Hospital Ethics Board and the Lanark, Leeds, Grenville Health Unit.
Tumbling TogetherTM Program
Tumbling TogetherTM is a gymnasium-based movement program for children 3 to 6 years of age with significant developmental and/or language delays. Continuous movement circuits and group activities are designed to meet individualized goals for self-regulation, sensorimotor/body control, group readiness, and language/communication. A small group of 6 to 8 children participate in each class. The activities performed during each class are led by a certified gymnastics coach, with individualized child support from a team of therapists (occupational therapist, speech language pathologist, communication disorder assistant, physiotherapy consultant) and trained therapy student volunteers. Each class begins with a group march into the gymnasium, followed by welcome songs as children sit in a circle. Subsequently, the children move through a circuit of gymnastic activities (e.g., jump on a trampoline, walk on a balance beam, swing on the uneven bars, roll on a slanted mat) that require various levels of strength, balance, coordination and self-regulation. Each time there is a transition between activities, the children line up and march as a group to the next activity. Each class ends with songs and circle activities to say “goodbye” and return the children’s energy and focus to leaving the class. Tumbling TogetherTM sessions were held in two locations, one a small city and the other a large town. Both locations were surrounded by primarily rural areas, where family income was known to vary widely. These locations for program delivery were selected to facilitate the participation of all children in need of the intervention, regardless of urban/rural location, socioeconomic status, etc. Parents accompany their child to the 45 minute class, but view the activities from outside the gym area. A trained parent educator supports parents to provide consistent expectations for the children’s behavior outside of the Tumbling program and provides individualized tips for enhancing communication and self-regulatory skills. Although Tumbling TogetherTM is highly recommended by therapists and coveted by parents, it is supported only by anecdotal evidence.
Participants
To be eligible for Tumbling TogetherTM, children must be 3 to 6 years of age, identified as having language, motor or cognitive delays, and able to walk independently. Children with only behavioural/non-compliance issues or families requiring services primarily for parental support are excluded. All children accepted into the Tumbling TogetherTM program during the evaluation period (Sept 2013 to Jun 2014) were enrolled in the study. Parents and caregivers of referred children attended an orientation session to learn about the program and what their child’s participation would require. During the orientation session, research staff described the study goals and procedures, and emphasized that the study was an optional component of the program. Questions about the study were answered by the researcher during the in-person meeting, and also by phone or e-mail.
Participants in this study were both the children (n=27; Table 1) enrolled in Tumbling TogetherTM and their parents/caregivers. The children were 3.8 +/- 0.5 years of age (min: 3.1 years, max: 4.8 years), with most being boys (24/27, 89%) who spoke English as their primary language (25/27, 93%). All participants had been identified as having significant language and/or developmental delay requiring intensive rehabilitation services. Diagnoses of neurodevelopment, developmental, psychiatric, communication, or other delays had been confirmed in 20 (74%) of the participants. A decision on the specific diagnosis was still being determined for 7 children (25.9%) who were undergoing additional diagnostic assessments concurrent with their participation in Tumbling TogetherTM. Parents/caregivers were primarily mothers (24/27, 89%). Although at least one member of 82% of the participating households was highly educated (post-secondary degree), family income was diverse. More than two thirds of participants (70.4%) lived in rural areas of Eastern Ontario.
Procedures
a. Video recording
It was proposed that video recording of the Tumbling TogetherTM activities would facilitate accurate coding and scoring, enable the program sessions to continue without interruption, and allow for a detailed examination of each child’s response regardless of when the assessment tasks were performed. The video recordings were taken from a distance so that the camera and photographer remained outside of the program activity area. A wide angle lens was used to capture all of the participants throughout the program. No attempt was made to focus the camera on specific children or activities. All video recording analyses were completed by the same investigator (AF).
Tumbling TogetherTM activity sessions were recorded at baseline (first two classes) and at the end of the program (last two classes). Program leaders use the first two sessions to define each child’s baseline level of performance as the combined assessment of these two sessions provides a more accurate picture of the child’s self-regulation. For many of the participants and their parents the first session is so overwhelming that their true capabilities are not evident until they return to a more “familiar” program on the second day. Conversely, children with attention difficulties often have enhanced performance on the first day (when everything is new/unknown) but return to a more distracted state on the second day.
Anecdotal evidence from clinicians and parents of previous participants provides strong support for the effectiveness of the Tumbling TogetherTM intervention. We hypothesized that if the video recordings were an effective method for assessing a change in self-regulation among program participants, then the video recordings should provide evidence of improved performance when comparing video recordings collected at the start and end of the Tumbling TogetherTM intervention. Parent perceptions of their child’s ability to participate in group programs were also evaluated at baseline and post-program, using a published questionnaire (Social Skills Checklist), as a secondary assessment of the validity of the video recording procedure. Three components of self-regulation fundamental to children’s participation in Tumbling TogetherTM, and physical activity and educational opportunities in general, were selected for this evaluation: paying attention and responding to the leader’s direction (Stop-and-Go commands), ability to sustain the requested behavior (lining-up), and turn-taking (waiting for a turn). These three self-regulation skills are practiced during each Tumbling TogetherTM session because they represent core learning that the professionals leading the program believe are essential and foundational to children’s participation.
b. Respond to a Command
The “Stop-and-Go” trampoline task is included in each Tumbling TogetherTM session in order to enhance the child’s ability to understand and respond to a command from the program leader. One at a time, children jumped on the trampoline while the coach held a sign. On one side the sign was a red octagon (the universal symbol for “Stop”), and on the other side the sign was a green circle (a symbol for “Go”). Before jumping, children were instructed by the coach to start jumping when the sign was green, and to stop jumping immediately when the sign was red. The coach would switch between green and red at random intervals to reduce the child’s opportunity to anticipate the change. Children were given the opportunity to respond to 5 “stop” commands before ending the game and leaving the trampoline. To evaluate the children’s ability to respond to a command from the program leader, the number of jumps each child completed before coming to a complete stop after the stop sign was displayed was counted for each of the 5 trials performed by each child. The average number of jumps required to stop across the 10 trials completed during the first two classes was used as the baseline measure. The 10 trials completed during the last two sessions of the program were similarly evaluated to provide the post-program measure.
c. Respond to an Action Signal
During each Tumbling TogetherTM session, children are requested to line-up with peers in order to move from one activity to the next. Children were instructed to line-up with their peers, one behind the other, as soon as they heard the “line-up bell” ring. Prior to the activity and to facilitate the children’s understanding of the concept of lining-up, the children were shown a picture of children lining-up and how they were to respond at the signal was explained. Research staff recorded, using “yes” or “no”, whether each child was able to line-up without additional support each time the signal was given. Video recordings of the session were reviewed to confirm the accuracy of the Yes/No responses recorded during the session. Although children had to line-up multiple times during each session, only the first trial during each class was evaluated. The research team and Tumbling TogetherTM leaders agreed that the first trial each day would better represent a real-life situation, where an appropriate response would be expected on the first cue. The percentage of children able to line-up independently was calculated for the first two and the last two weeks.
d. Ability to Wait
Waiting for a turn is a fundamental self-regulation skill that is a focus of the Tumbling TogetherTM program because of its importance for safety as well as social interactions with peers. For this study, the child’s ability to wait for a turn was evaluated during a circuit of gymnastics activities. Children were instructed to wait on designated floor mats before the first activity in the circuit. When it was safe for them to go (e.g. area clear, no child in front of them) they were given a signal to begin the first element of the circuit. Video recordings of the circuit activity were reviewed by the researcher (AF) to determine whether or not the children had waited for their turn (yes or no). If the child left the waiting floor mat before the signal to begin was given, or if the child required additional support from program staff (e.g. verbal prompts, visual (pointing), repetitions or physical manipulation) in order to wait, they were rated as “not able” to wait.
e. Social Skills
Parent perceptions of their children’s social skills were evaluated using the Social Skills Checklist (Elementary/Pre-K) [17]. The Checklist is comprised of 66 questions within 3 categories: a) social play and emotional development, b) emotional regulation, and c) communication skills. Social Play & Emotional Development examined beginning play behaviors (e.g., proximity or imitation of peers, 6 items), intermediate play behaviors (e.g., sharing toys, taking turns, greeting peers, 8 items) and advanced play behaviors (e.g., cooperative play, offering toys to peers, 6 items). Emotional Regulation assessed understanding of emotions (e.g., identifies emotions, interprets body language, 10 items), self-regulation (e.g., comforted by others, accepts being told “no” or not being first, 11 items), flexibility (e.g., accepts mistakes with upset, accepts unexpected changes, 5 items) and problem solving (identifies problems, generates solutions, 4 items). Communication Skills assessed verbal conversational skills (e.g., initiates conversation , asks “wh” questions (who, what, where etc.), 8 items), non-verbal conversational skills (e.g., orients to speaker, waits to interject, 4 items) and compliments (e.g., appropriate comments to peers, apologizes independently, 4 items). For each question, parents indicated the frequency with which their child performed each social skill on a 4-point Likert scale (Almost Always, Often, Sometimes, or Almost Never). Parents completed the Checklist during the first week of the Tumbling TogetherTM program (baseline) and then again during the second-last week of the program (post-program evaluation). Points were assigned to each response: 1 = Almost Always, 2 = Often, 3 = Sometimes, 4 = Almost Never. Average scores were calculated for each sub-category, with a lower score indicating that the child demonstrated the social skill more often.
Data Analyses
Chi-square analyses evaluated whether the children’s ability to wait (Yes/No) or response to an action signal (line-up) changed after program participation (baseline/post-program). Paired t-tests evaluated changes in command response (# of jumps to stop) and social skills scores. All analyses were completed using SPSS statistical software (Version 21).
RESULTS
Video images were suitable for the analysis of child performance during all recorded Tumbling TogetherTM sessions. There was no evidence that the presence of the camera and photographer was a distraction to the participants (e.g., no images of children staring at the camera or running toward the photographer).
Respond to Command or Action Signal
Children significantly improved their ability to respond either to a “stop” command or an action signal (line up) after participating in Tumbling TogetherTM (Table 2). Children were able to understand and respond to the stop signal 38% faster while jumping on the trampoline. The proportion of children able to independently line up in response to the action sign (bell ring) increased from 26% to 89%.
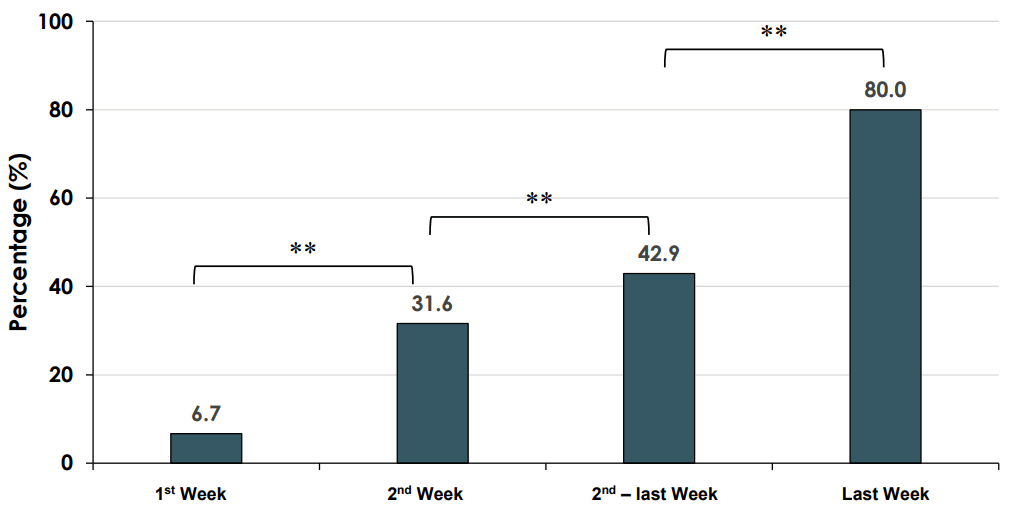
Ability to Wait
Children’s ability to wait improved throughout the program sessions (χ2 = 29.9, p = .001). Compared to the first session of the program (7% able to wait), the percentage of children who were able to wait before starting the circuit during the last session (80%) was more than 13 times higher (Figure 1).
Parent Perception of Social Skills
Parents reported a broad range of social skill improvements among children attending Tumbling TogetherTM (Table 3). Intermediate (t = 3.8, p = .001) and Advanced Play Behaviors (t = 3.8, p = .001), such as returning and initiating greetings with peers and playing cooperatively with peers during imaginative play, became more frequent. Understanding Emotions (t = 2.4, p = .02), such as demonstrating affection and empathy towards peers, and Self-Regulation (t = 3.9, p = .001), such as saying “no” in an acceptable way to things the child does not want to do, also improved. Flexibility (t = 3.3, p = .003), such as accepting unexpected changes, Problem Solving (t = 2.5, p = .02), such as understanding the impact of his/her behavior on peers, Conversational Skills (t = 3.4, p = .003), such as introducing him/herself to someone new, and Compliments (t = 3.6, p = .002), such as apologizing independently, also improved significantly. Parents did not report any improvements in Beginning Play Behaviors (t = .5, p = .6) or Nonverbal Conversational Skills (t = 1.4, p = .2). These skills would include the ability to maintain proximity to peers and orient the body towards the speaker.
DISCUSSION
Tumbling TogetherTM is a physical activity-based intervention program that targets both self-regulation and communication skills. The gymnastic-based activities are designed to be fun and exciting; engaging and motivating the children to acquire the skills needed for successful participation. Enabling parents to watch their children’s participation, as well as staff responses to inappropriate behaviors, is hypothesized to provide a positive model. Although anecdotal evidence from program leaders, therapists and parents strongly supports the efficacy of Tumbling TogetherTM, objective evidence regarding the impact of the program was lacking. The dynamic nature of exercise-based interventions and the self-regulation limitations of the young participants posed unique challenges to the implementation of standardized outcome assessments. This study evaluated whether digital video recordings of the intervention sessions could provide objective, measurable evidence of the impact of the Tumbling TogetherTM intervention.
Attending Tumbling sessions improved children’s self-regulation skills as evidenced by measurements obtained from the session video recordings of their increased ability to line up on command, respond to leader directions, and wait for a turn during activities. The improvement in parent ratings of their child’s social interactions, emotional regulation and conversational skills over the intervention period provides further evidence in support of the validity of the measurements extracted from the video recordings. These improvements in self-regulatory skill would be expected to facilitate the children’s participation in school and community programs. The ability to anticipate appropriate responses (e.g. knowing how to line up when requested), pay attention to the teacher (e.g. trampoline stop and go), keep calm during instruction time, interact and play with classmates, share toys and supplies, and inhibit impulsive behaviors (e.g. wait for turn) are essential for successful peer interactions [18]. Similar play-based interventions have previously been reported among healthy children of preschool age [19] and children living in low income families [20].
Given the difficulty of implementing meaningful but standardized assessments of self-regulation in preschool children with developmental delays and behavioral issues, the existing body of evidence is very limited. Published evidence supporting the efficacy of interventions to enhance self-regulation is limited to school-age children. Self-monitoring, self-management, and self-reinforcement interventions improved on-task behavior, reduced inappropriate behavior, and enhanced academic accuracy and productivity among children with attention deficit hyperactivity disorder [21]. Exercise interventions have been shown to enhance academic performance and reduce self-stimulation among school-age children with autism [22]. A movement-based horseback riding intervention also demonstrated significant improvements in behavior and social communication among school-age children with autism spectrum disorder [23]. Our video recording methodology enabled us to evaluate similar behaviors among younger children, including the ability to self-monitor (e.g. trampoline stop and go) and self-manage (e.g. wait for turn, line up).
From a developmental perspective, self-control is an initial phase of self-regulation that is characterized by compliance and the ability to behave according to caregiver or social expectations even when external sources of control (e.g. parent oversight) are absent [24]. As the development of self-regulation becomes more advanced, the child develops the ability to maintain self-control in spite of changes in the environment [24]. In this study, video recordings were used to assess primarily tasks requiring self-control (lining up or stopping on command, waiting for a turn), since the Tumbling TogetherTM sessions were delivered in a consistent environment (e.g. same staff, equipment and activities each week). However, the flexibility and portability of digital video cameras suggests that recording children’s involvement in a variety of settings could be similarly feasible, which would also enable the evaluation of more advanced selfregulation capacities. Future research should investigate the impact of the Tumbling TogetherTM exercise intervention in a randomized controlled trial. The validity of using the video recording technique to evaluate participants’ self-regulation within a variety of environments (e.g. community gymnasium, home, child care or school) should also be evaluated through future research.
Limitations
In this study all participants attended the Tumbling TogetherTM program. Whether the gains achieved would be similar for a control group not receiving the intervention remains unknown. Future research that measures self-regulation within and outside of the Tumbling TogetherTM program would more clearly indicate the generalizability of these results. Due to limited program capacity and availability, the number of study participants was relatively small (n=27) even though all children attending the Tumbling sessions were enrolled in the research study. There was a maximum of 8 children per session, with the number of sessions offered restricted by a lack of funding. Participating children were mostly male, with the study having only 3 female participants. The differential sex distribution of program participants reflects the relatively higher prevalence of autism and developmental disabilities among males [25]. These results must also be considered in light of the fact that all Tumbling TogetherTM sessions were led by the same staff. Additional research is required to determine whether the same program administered by different leaders would achieve equivalent results.
CONCLUSIONS
This study determined that video recording an exercise intervention, Tumbling TogetherTM, enables an evaluation of indicators of self-regulation among preschool-aged children with developmental delays or behavioral issues. Changes observed in children’s communication and social skills identified on the video recordings were similar to parent reports of the child’s capacities. The video recording methodology should be further evaluated in future studies comparing children who do and do not receive the Tumbling program, with the video recordings evaluated by multiple examiners, as well as the use of video recordings to evaluate children’s self-regulation within a variety of environments.