



INTRODUCTION
In recent years high-intensity interval (HIT) exercise has been widely spread in athletic exercise training. HIT is known as a time efficient training regimen improving not only endurance performance[1,2] or oxygen uptake[3] but also arterial stiffening[4,5], lipid oxidation[6] and insulin sensitivity[7]. Due to these benefits HIT was started being transferred from exercise training into prevention and rehabilitation for patients especially in the field of cardiovascular disease and diabetes[8–14]. An important marker and risk factor of cardiovascular disease amongst others (e.g. hyperglicemia, blood pressure, obesity, etc.) is arterial stiffening. Physical activity and exercise training has been shown to improve the prevalence and ameliorate the progression of arterial stiffening and metabolic derangements closely linked to vascular structure and function[14–17]. Atrial natriuretic peptide (ANP) is a member of different natriuretic peptides secreted by the heart in response to pressure overload and myocardial stress. ANP is one of the vasodilating substances being increasingly released with rising physical work[18,19] Notably it also exerts metabolic action including lipolysis and lipid oxidation[20]. When comparing HIT and continuous exercise (CE), HIT has comparable beneficial effects on improving arterial stiffness[21]. Tordi et al.[22] suggested this could be due to a higher release or production of vasorelaxing substances such as lactate or atrial ANP. However a recent study of Peres and colleagues [23] did not find significant differences in ANP between HIT and CE. Other studies have shown correlations between changes in ANP, heart rate (HR)[24] and exercise intensity[25]. As there are opposing outcomes of studies in the recent literature, the knowledge of ANP in conjunction with HR, physical work and different interval protocols needs to be extended. In case of HR we did not find differences for HR between different High Volume High Intensity Training (HVHIT) and continuous exercise (CE) regimens with matched mean intensity[26]. With the current study we seek to extend the knowledge of ANP-release through different interval and continuous exercise protocols (HVHIT, HVSIT, CE). Since the active form of ANP is reduced by the clearing through natriuretic peptide receptor C (NPR-C) and neprilysin, mid-regional-proANP (mr-proANP) a precursor molecule of ANP is a more stable biomarker in blood and ex vivo[27]. Mr-proANP is released in an equimolar ratio as ANP[27], thus it provides a reliable biomarker for ANP release by the heart[28]. Thus we conducted a study with two different HVHIT protocols and a CE to compare and evaluate physiological effects in regard to plasma mr-proANP-concentrations and metabolic reactions before and immediately after the mentioned exercise regimens.
METHODS
Subjects
Six healthy subjects (VO2peak 4.3 (±0.5) min*l-1, range 3.6 - 5.1 min*l-1; PmaxGXT 4.2 (± 0.4) W*kg-1, range 3.8 – 4.8 W*kg-1; weight 81.4 (±10.2) kg, range 68.1 – 95.9 kg; height 182.8 (±5.8) cm, range 175 – 192 cm; age 28.3 (±6.4) y, range 22 – 41 y) were recruited for the study. Inclusion criteria: Male, 18 y or older, healthy, recreational active in endurance or team sport (2 – 4 training sessions per week). Exclusion criteria: acute or chronic inflammation, other acute or chronic pathologies preventing subjects from participating in physical exhaustive exercises, drug and alcohol abuse. Subjects were asked to refrain from any diet during the study and keep their standard nutrition habits. All subjects were enlightened about benefits and risks regarding all study procedures. All study procedures were approved by the local ethics committee of the Hannover Medical School (IRB number 6149) and all subjects gave their informed written consent beforehand of any study procedures. All study procedures fully applied to the ethical standards of the Helsinki Declaration. No subjects under age of 18 years were included in the study.
Exercise Testing
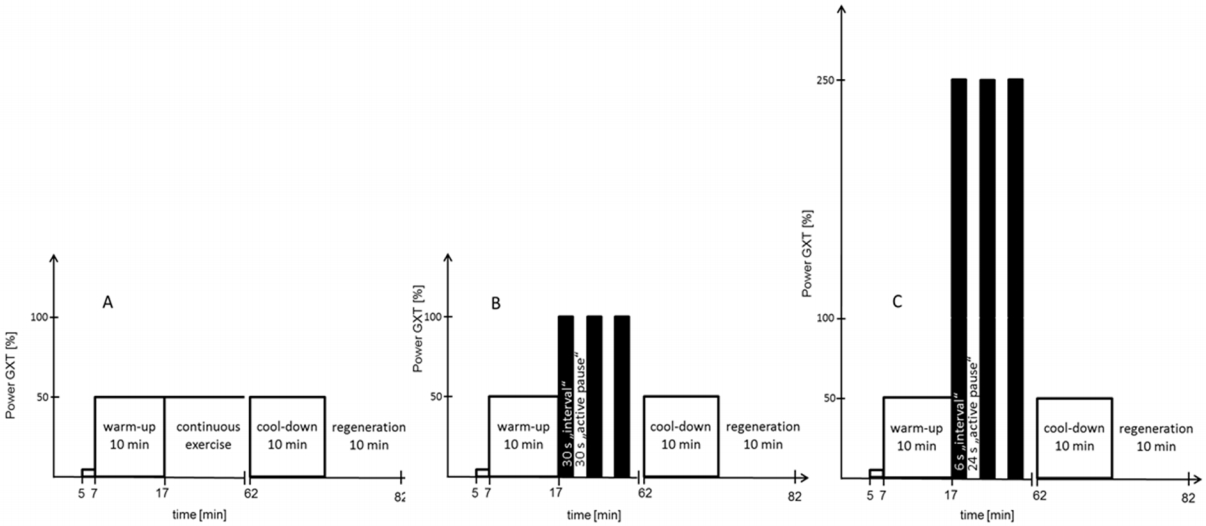
Methods have been described before[29]. In brief: All tests and training sessions were performed on a Lode Excalibur cycle ergometer (Groningen, The Netherlands). A graded exercise test with 16.6W increments per minute (GXT) was carried out to test for VO2peak and maximum power output (PmaxGXT). Spirometrical data was recorded breath-by-breath using a Metalyzer 3B (Cortex Biophysik GmbH, Leipzig, Germany). After the GXT a continuous training (50% PmaxGXT) (CE), a high volume high intensity interval training with 30s load (100% PmaxGXT) and 30s pause (HVHIT) and a high volume sprint interval training with 6s load (250% PmaxGXT) and 24s pause (HVSIT) was completed by every subject in randomized order (Figure 1). Subjects performed active pause with 10W and cadence between 80 and 100rpm. To keep mean intensity during exercise at 50% Pmax, intensity during interval phases was adjusted proportionately (-10W for HVHIT and -40W for HVSIT). Proportionately intervals and active pauses result in a mean intensity of 50% PmaxGXT. All tests and trainings were seperated by 48h – 96h.
Blood Samples
During CE, HVSIT and HVHIT venous blood samples from an antecubital vein were drawn. EDTA was used as anticoalugation. Blood samples were immediately centrifuged at 4°C, plasma was aliquoted and deep frozen at 80°C for later mr-proANP analysis. Mr-proANP was analyzed using a sandwich immuno- assay in a chemiluminescence coated tube format (BRAHMS AG, Hennigsdorf/Berlin, Germany) as described by Morgenthaler et al.[30].
Venous blood samples for Na and K+ were immediately analyzed using an ABL Flex 800 (Radiometer, Krefeld, Germany).
During all tests capillary blood samples were drawn from an earlobe. Earlobes were hyperaemized with Elacur M Hot Crème (Carinopharm GmbH, Elze, Germany) before the first sample was drawn. Capillary blood was drawn into a 20µl end-to-end capillary. Filled capillaries were mixed with glucose/lactate hemolyzing solution (Biosen, EKF Diagnostics) and analyzed within the next two hours. ReadyCon pat/norm/multi standards (Biosen, EKF Diagnostics) were used for analysis.
Statistical Analysis
All figures containing spirometrical data display 60s mean values. For statistical evaluation of spirometrical data mean values of 60s were used. All values are given in means ± standard deviation (SD). Statistical significance was set to p<0.05 and all analyses were two-tailed. Data was tested for normality using the Shapiro-Wilk-Test. Due to the crossover design of the study analyses for detecting possible differences between CE/HVSIT/HVHIT were made using repeated measurement one way analyses of variance (RM ANOVA). To adjust for multiple comparisons post-hoc test Holm-Sidak was applied with all RM ANOVA testing when significant interactions were detected. No outliers were removed from the calculations. Data sets of all subjects have been complete. To detect significant correlations linear regression (f = y0+a*x) analyses were carried out.
RESULTS
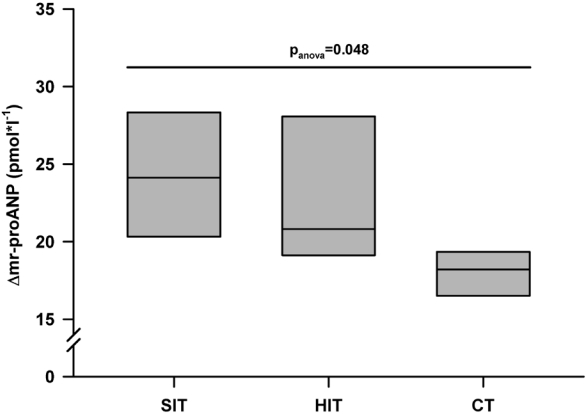
Statistic calculation revealed an overall significant difference between HVSIT (25.5±7.8 ρmol*l-1), HVHIT (22.5±4.5 ρmol*l-1) and CE (17.8±2.0 ρmol*l-1) for Δmr-proANP with p=0.048 (Figure 2.). Post-hoc testing showed that HVHIT was significantly different (p=0.018) to CE, but HVSIT/CE (p=0.076) and HVHIT/HVSIT (p=0.422) weren’t significantly different.
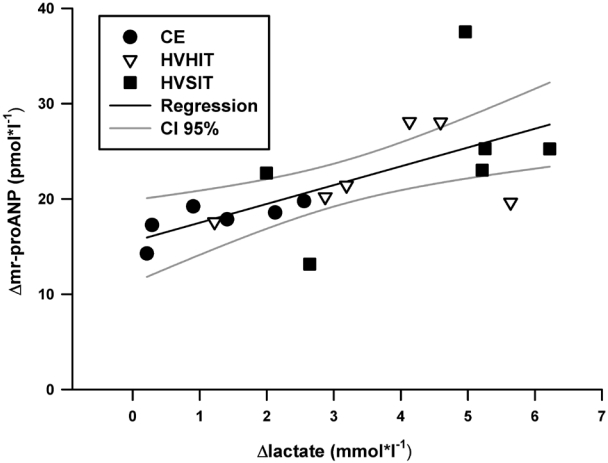
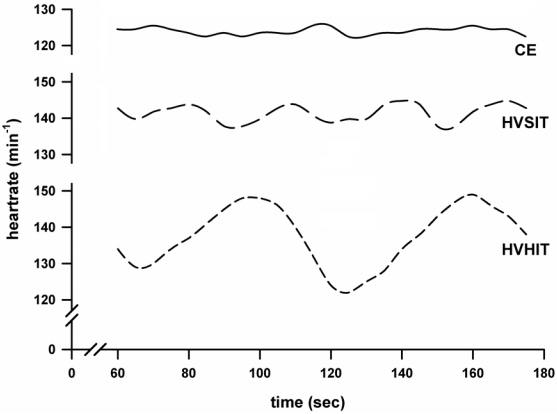
Maximum heartrates at the end of exercise (HVHIT 160 (±5.1) min-1; HVSIT 163.1 (±3.0) min-1; CE 157.1 (±5.7) min-1) were not significantly different between the three exercise protocols (p=0.58). VO2peak reached 3.2 (±0.2) ml*kgBW-1 during HVHIT, 3.1 (±0.2) ml*kgBW-1 during SIT and 3.1 (±0.1) ml*kgBW-1 during CE. VO2peak was not significantly different between the three exercise regimens. [Lac] was significantly higher (p>0.01) in HVSIT and HVHIT compared to CE. [lac] during SIT reached 5.1 (±0.62) mmol*l-1, 5.2 (±0.48) mmol*l-1 during SIT and 2.6 (±4.41) mmol*l-1 during CE. Between HVSIT and HVHIT no significant differences were found (p>0.05) for [lac]. [Δ lac] had a significant positive correlation with [Δmr-proANP] (R=0.654; p=0.003; Figure 3) and a negative correlation with [ΔK+] (R=-0.471; p=0.048). No other significant correlations with P, Na, VO2peak or HR were found. However, in Figure 4, we display the courses of HR during the respective exercise regimen. Although the means are not significantly different between the three exercises, the heartrates are showing characteristic courses in the respective exercise regimen.
DISCUSSION
In this study we conducted a high volume high intensity interval protocol, a high volume sprint interval protocol and a continuous exercise protocol with matched mean intensity. We measured plasma mr-proANP-concentrations, lactate, HR and VO2 to extend the understanding of possible beneficiary effects of interval exercises on arterial stiffening compared to continuous exercise. Δmr-proANP was significantly different between HVHIT, HVSIT and CE suggesting a different ANP-release amongst the different exercise protocols.
∆mr-proANP was highest in the SIT protocol which had the highest absolute and delta lactate-concentrations. However only ∆lac yielded a significant correlation to ∆mrproANP suggesting a relationship of lactate production and ANP-release. This strengthens the hypothesis of Tordi et al.[22] that HIT triggers a higher ANP-release compared to continuous exercise. In contrast Peres et al.[23] found no significant differences in ANP between interval training (IT) and CE. Reasons for these opposing results might be that Peres et al. measured ANP directly and not through mrproANP as a marker of ANP-release. ANP is being reduced through the NCP-R pathway permanently and mr-proANP is not. Although we can’t exactly seize the magnitude of this effect it could be a reason for the differential outcomes. Additionally Peres and colleagues used a different interval protocol with substantially longer interval and pause lengths. In 45 min of exercise only 5 intervals (1 min length) were allocated compared to 45 (HVHIT) or 90 (HVSIT) intervals during 45 min in our study.
Differences of FFA and glycerol remained insignificant in our previously published results[29] between HVHIT, HVSIT and CE. Since ANP was shown to stimulate lipid mobilization[31] this does not align with results in the literature. Additionally mr-proANP did not correlate with FFA or glycerol thus we suggest either a reduced impact during strenuous exercise or a different reduction of ANP during exercise. Based on the small sample size we do not want to make a definite statement on these opposing results, since beside ANP duration of exercise, mean intensity, glycogen loading and concentration of insulin and catecholamine can influence lipid oxidation during exercise. Thus one reason for the missing correlation might be the numerous factors influencing lipid oxidation.
Interestingly other studies[18] have shown correlations between power or physical work and ANP-release, but in our study this correlation was not apparent. Our study did match mean intensity using Pmax from a graded exercise test to be exact 50% of Pmax in all exercise regimens. However absolute intensities did differ during interval phases, but still absolute intensities did not significantly correlate with mrproANP or ∆mr-proANP. A positive significant correlation was found for ∆mr-proANP and ∆lac. Up-to-date there are no studies presenting results that lactate metabolized by the heart could be an additional factor influencing ANP-release. There are results suggesting an involvement of HR or venous blood flow[32]. Due to our small sample size correlations have to be interpreted with care in our study and we could only speculate if there is a mechanistic relationship between lactate an ANP. However the regression analyses did show a promising correlation. Additionally as ANP is known to be released due to the mechanical stress following a volume expansion and atrial pressure in the heart[33,34], ANP-release should be enhanced by the intermittent nature of HVHIT or HVSIT training through the generated atrial pressure changes. In Figure 3 we display the heartrate (5s means) over the course of 2 min during exercise (HVHIT, HVSIT, CE). It is seen that during HVHIT the amplitude of the heartrate is the highest amongst the evaluated exercise regimen. But the highest ∆mr-proANP in this study is seen during HVSIT. Thus we speculate that the atrial pressure changes are elevating the ANP-release during HVHIT and HVSIT compared to CE, but there should be additional factors influencing ANP-release. More research with better sample size will be needed on this issue.
Limitations
The study is limited by the small number of subjects. Thus we interpreted our results with care. A generalization would not be applicable. However based on the repeated measurement design of the study we do have a sufficient sample size to have acceptable power in our analyses to detect significant differences in our outcomes. Additionally since we measured mr-proANP we can not be sure of actual ANP-levels in plasma. However mr-proANP provides a valid marker for ANP-release by the heart. Thus the ANP-release following the different exercise regimen can be evaluated reliably.
CONCLUSIONS
We conclude ANP-release is different in higher volume, high intensity exercises compared to continuous exercise. ANPrelease is influenced by atrial pressure changes, but based on our results there could be additional factors elevating ANP-release during exercise. Intermittent training might be a feasible strategy to enhance ANP levels and thereby improve cardiovascular as well as metabolic risk particularly in individuals with relative natriuretic peptide deficiency.