Participation in a Community-Based Sport Program is Feasible for Children with Congenital Heart Disease and May Benefit Physical Literacy Development: A Pilot Study
Article information

Abstract
OBJECTIVES
Children with congenital heart disease (CHD) often lack confidence and demonstrate limited movement skills during physical activity. Community-based sport programs have been suggested to build their confidence and competence. This study examined the feasibility and physical literacy impact of an existing community-based sport program for children with moderate to complex CHD.
METHODS
This pilot study employed a parallel mixed method, single-case experimental design to evaluate the feasibility and impact of a weekly, community-based sport intervention (Sportball©). Intervention field notes and focus group transcripts were analysed deductively to inform feasibility. Physical literacy outcomes were measured using the Canadian Assessment of Physical Literacy. Paired t-tests examined changes in physical literacy scores, while qualitative data informed perceived changes in physical literacy tasks.
RESULTS
Participants (n=11, 45% female) were 8.2 ± 1.2 years. Nine children completed >80% of the 1-hour Sportball© sessions (10 lessons total). No adverse events occurred during or as a result of the intervention. Enabling participants to recognize the sensations of exercise and whether or not they needed to rest, designing activities and instructions to mitigate the risk of body contact, and accommodating the needs of participants with developmental/attentional limitations were important factors embedded into the design of the program, contributing to its feasibility. Participants reported perceived improvements in movement skill and torso endurance/strength, changes which were reflected in the objective physical literacy measures (movement skill: ∆ mean= 2.0 ± 0.98 points, p=0.07, r=0.57; torso endurance/strength: ∆ mean= 5.27 ± 7.20 seconds, p=0.44, r=0.26).
CONCLUSIONS
The Sportball© intervention was feasible for children with CHD, including those with activity restrictions or developmental delays. Children enjoyed the program and wanted it to continue. Measurable improvements in movement skill and muscular endurance were recognized by participants. Future trials evaluating Sportball©’s impact with larger samples and multiple 10-week sessions are recommended.
INTRODUCTION
Physical activity participation (including sport) is central to childhood health [1] and quality of life [2]. The development of physical literacy is necessary for active participation and is defined as “the motivation, confidence, physical competence, knowledge and understanding to value and take responsibility for engagement in physical activities for life” [3]. Adopting an active lifestyle is particularly important for children with congenital heart disease (CHD), who face a greater risk of developing secondary chronic disease as a result of sedentary lifestyles [4]. In Canada, where approximately one in every 100 children is born with CHD [5], community sport programs are widely available and may offer accessible, diverse opportunities for children with CHD to build active lifestyles [6]. However, healthcare providers often hesitate to recommend recreational sport programs to their patients with CHD, given the paucity of evidence supporting their safety and efficacy [7].
Inactive lifestyles observed among children with CHD are hypothesized to reflect low levels of physical literacy. Children with CHD face unique physical activity barriers [8] and medically necessary activity restrictions [9]. More specifically, children with CHD have a high prevalence of motor skill and developmental delays [10], as well as reported cognitive [11] and physiological [12] barriers limiting their physical activity (i.e. low cardiorespiratory fitness). Since physical activity self-efficacy and exercise capacity are positively associated with activity participation [13], physical literacy and the components which inform it (i.e., physical competence, motivation, etc.) are salient outcomes for children with CHD.
This pilot study sought to evaluate the feasibility of a widely available community-based sport program (Sportball©) among children with moderate to complex diagnoses of CHD [14]. Sportball © is a multi-sport program which aims to develop children’s physical literacy and sport-specific skills. Each session focuses on a different sport and includes warm-up and cool-down activities, individual skill progressions and cooperative games. It was hypothesized that Sportball© would be appropriate for children with CHD, despite restrictions due to their cardiac diagnosis. A secondary objective of this study was to evaluate the impact of Sportball© on physical literacy outcomes, with hypothesized improvements in motivation, confidence, physical competence, and physical activity behaviour.
METHODS
A parallel mixed method, single-case experimental design was used for this pilot feasibility study. Since both physical and psychosocial factors relating to participation in sport are complex, the combined use of quantitative and qualitative data in this convergent design was chosen to provide a pragmatic and comprehensive evaluation of the intervention [15]. Focus groups and physical literacy assessments were both performed 1-week before and following the 10-week intervention (Table 1). This study was approved by the research ethics boards of the children’s hospital (IRB#16/61X).

Study Design
Study Participants
Participants with moderate to complex diagnoses of CHD (i.e., requiring invasive, surgical intervention with on-going follow-up) [14] were selected using non-probability, purposive sampling by age (7–10 years), sex (male/female balance) and geographical location (Ottawa and surrounding area). Potential participants were excluded if they had undergone cardiac surgery or catheterization in the previous 6 months or if they had been diagnosed with a medical condition known to significantly impair motor development (i.e., Down syndrome, cerebral palsy). Eligibility and medical history were determined using an electronic health record. Following parent and participant consent, the responsible cardiologist was asked to specify medically necessary activity restrictions.
Intervention Design
An existing community-based program (Sportball©; www.sportball.ca) was chosen for this study due to its rigorous structure, replicability, and wide availability across North America. Participants were asked to meet at a community facility once per week, over a period of 10 weeks for the 1-hour/week intervention. All sessions were facilitated by the lead researcher with support from an experienced Sportball© coach. Participants attended the intervention in either fall 2016 or winter 2017. Both interventions were identical in terms of program delivery. Participants were considered to have experienced the full intervention if they attended at least 80% of the 10-week session (i.e., 8 classes). Each session followed a pre-determined lesson plan: a 10-minute warmup, instruction of 2 to 3 sport-specific skills, 1 or 2 cooperative team games, and a 5-minute cool-down.
Data Collection
a. Field Notes and Focus Groups
Data obtained from field notes and focus groups contributed to assessing the feasibility of the intervention. Field notes were completed by the lead researcher immediately following each Sportball© session. These notes provided detailed records of changes to the Sportball© protocol (i.e. exclusion of activities), participants’ progression and completion of skills, as well as attendance and reasons for absence. Occurrences related to the various domains of physical literacy (i.e., motivation, competence, etc.), including relevant interactions between participants and their environment, were also noted.
Focus groups were facilitated by the researcher during the fall 2016 session. A sub-sample of participants was purposively selected based on age (8 to 9 years), as it is recommended that children participating in focus groups should be no more than 2 years apart [16]. Each focus group (~35 to 40 minutes) was held in a room at the community centre where the intervention was delivered, and parents attended focus groups to enhance the comfort of participating children. Both focus groups followed a semi-structured interview guide and were audio-recorded. Focus group data provided additional information about how participants perceived their physical literacy.
b. Physical Literacy Assessment
Participants completed the Canadian Assessment of Physical Literacy (CAPL), a valid, reliable, and comprehensive tool for evaluating the physical literacy of children [17]. Raw scores obtained from each test were assigned a composite score. Composite scores for each of the 4 domains (i.e., physical competence, knowledge/understanding, daily activity, and motivation/confidence) were summed to determine an overall CAPL score (out of 100 total points). For each domain, as well as the total CAPL score, the numerical score is placed into 1 of 4 classifications based on normative data adjusted for age and sex, describing a child’s physical literacy journey as beginning, progressing, achieving, or excelling.
The physical competence domain in the CAPL includes measures of musculoskeletal fitness, body composition, gross motor skill, and cardiorespiratory endurance [17]. Measures of static grip strength, trunk and hip flexibility, and torso muscular endurance (a timed plank hold) were used to determine musculoskeletal fitness. The Canadian Agility and Movement Skill Assessment (CAMSA) was used to measure gross motor skill [18]. The CAMSA combines assessments of skill execution and completion time that evaluate fundamental, complex, and combined movement skills. A 15-meter shuttle run test (PACER) was used to measure cardiorespiratory endurance [19]. A more detailed description of the CAPL can be found at www.capl-ecsfp.ca.
Objective measures of daily activity were taken throughout the study, at weeks 1 (baseline), 4, 8, and 12 (post-test). An omni-directional, Actical Z-series accelerometer (Respironics, USA), set to 15-second epochs, was worn by each participant. Daily physical activity includes all physical movement, such as leisure activities (i.e. extracurricular sport) and activities of daily living. Participants were therefore instructed to wear the accelerometer over their right hip during all waking hours, for a period of 7 consecutive days. The accelerometer recorded activity intensity, duration, and step counts. Valid days had at least 10 hours of recorded data, while a valid week included a minimum of 3 valid weekdays and 1 valid weekend day.
Data Analyses
a. Qualitative Analyses
Focus group and field note data were viewed from an interpretivist epistemology, which considered unique life experiences (i.e., medical history, perceived health concerns), to better understand the feasibility of the Sportball© intervention. Audio recordings from focus groups were transcribed verbatim, and pseudonyms were used to maintain participant confidentiality. Braun and Clarke’s six steps for thematic analysis [20] were deductively used to identify key themes on feasibility, based on known barriers to PA participation. Focus group data pertaining to participants’ physical literacy (i.e. completion of CAPL) were used to evaluate convergence between perceived and observed changes in physical literacy outcomes.
b. Statistical Analyses
Descriptive results from the CAPL are reported in mean differences ± standard error. Paired t-tests were used to examine changes in raw CAPL scores and physical literacy outcomes between pre- and post-intervention, with significance at p<0.05. Where skewness or kurtosis were observed, Wilcoxon signed rank tests were used instead. Complete scores for each CAPL domain were required from participants at both pre-test and post-test in order for those participants to be included in the statistical analyses of the relevant domain. A repeated measures analysis of variance evaluated changes in daily time spent in moderate-to-vigorous physical activity throughout the study period. Effect sizes and 95% confidence intervals were reported where applicable to indicate the variability of the outcomes and degree of potential change. Small and medium effects were indicated by r >0.3 and r >0.5, respectively. Sensitivity analyses [21] were performed to account for any difference in results due to attendance (i.e. less than 80% of the intervention). All statistics were run using SPSS (Version 25.0).
RESULTS
Participants
A total of 11 participants were enrolled in this pilot study. One participant (9%) withdrew halfway through the winter session to receive treatment for an unrelated medical condition. Two participants (18%) in the fall session refused to complete post-intervention questionnaires (assessing knowledge and motivation) but did complete the physical competence outcomes (Table 2). Thus, 8 participants were included in most statistical analyses (38% female), with the exception of physical competence outcomes (n=10; 48% female). Table 2 provides descriptive data of all participants enrolled and for those who completed study tasks (i.e., CAPL, physical competence). Of those with complete physical competence scores, only 1 participant did not complete the intervention as intended (i.e. attended <80% of sessions). Participants were between the 15th and 85th percentiles for height and between the 25th and 75th percentiles for weight, except for 2 participants (18%) who were above the 97th percentile for weight [22]. A subset of 4 children (50% female) participated in focus groups during the fall session.

Participant Demographics and Physical Activity Restrictions
Feasibility
Of the 28 eligible participants approached to participate, reasons for declining were unrelated to the child’s CHD (distance=6, scheduling=2, child was already active=4, disinterest=5). Of the 11 participants enrolled, 82% (n=9) attended the majority of the Sportball© sessions (i.e. >80% of sessions). No adverse events occurred during or as a result of the intervention. Reasons commonly cited for absence included: illness (n=6), scheduling conflicts (n=2) or difficulties traveling to the study location (n=3). In order to recruit enough participants for the winter 2017 session, siblings were welcomed to join the program if they were within the same age range (i.e. 7–10 years), which did not impact the delivery of Sportball©.
All participants remained engaged throughout the intervention, and most participants (n=9) frequently mentioned their enjoyment of Sportball©. The structure of the program, variety of sports played, and feelings of inclusion among peers contributed to the perceived enjoyment of the intervention. Main themes highlight relevant factors to consider when delivering a community-based sport intervention to participants with CHD. They include: 1) understanding self-regulation and accommodating the need for rest; 2) adapting activities and participant instructions to mitigate the risk of body contact; and 3) understanding and addressing the needs of participants with developmental and attentional limitations.
Understanding Self-Regulation and Accommodating the Need for Rest
Participants recognized and communicated their perceived level of exertion and fatigue. For example, John (age 8) held his chest following some running activities and would either take a short break or maintain participation stating he was “just tired”. Many other participants (45%) took breaks after running. One focus group participant recalled feeling “exhausted” during Sportball©. Although some participants showed more symptoms of fatigue than others, none demonstrated signs of over-exertion (hyperventilation, disorientation, chest pain, difficulty speaking, heavy perspiration). Activity adaptations were used to decrease intensity and encourage further participation (i.e. skipping or sliding instead of running). A 5-minute break occurred during every session, as per the Sportball© protocol. While additional breaks taken by participants were infrequent (i.e. no more than 2 breaks per session), they were always permitted and did not interfere with the delivery of the program. Participants were never excluded from engaging in an activity if they required a break.
Mitigating Risk of Body Contact
The only sport excluded from the Sportball© sessions was football, given hard bodily impacts are embedded into the objectives of the game. This exclusion did not detract from the objectives of the intervention (i.e. skill development) and was introduced to accommodate medically necessary restrictions for children who had pacemakers (n=2) or anatomical abnormalities (n=1; chest wall deformity). Nevertheless, bodily impacts still occurred. For example, some participants used unnecessary force to obtain the ball (i.e., pushing, pulling) during basketball. Participants were also observed colliding with one another unintentionally during the first 4 lessons. Coaches responded by delivering more frequent, explicit instructions to avoid contact, and as a result, no significant impacts were observed during the following lessons.
Understanding and Addressing the Needs of Participants with Developmental and Attentional Deficits
More than half of study participants (n=6) had been diagnosed with a developmental delay or attention deficit hyperactivity disorder (ADHD), which sometimes challenged the completion of session activities. For example, during the tennis lesson participants were shown how to use the racquet to manipulate various objects (i.e., bean bag, small ball) for ten consecutive hits. Some (n=2) participants with diagnosed deficits did not work towards the instructed goal of consecutive hits, despite repeated guidance from coaches. Understanding of the intervention activities also varied. John (age 8; mild intellectual delay, ADHD) achieved sport-specific skills but struggled to perform functional exercise movements. Contrarily, Peter (age 7) had similar intellectual delays but found it difficult using sportspecific terminology. Coaches were trained by Sportball© to respond to the needs of children with diagnosed delays by exercising patience and providing multiple variations or explanations of activities that would meet the skill levels of all participants. Although neurodevelopmental limitations may have influenced participants’ understanding of each lesson, they did not hinder participation as the group remained engaged throughout the intervention.
Physical Literacy
There was no difference in total CAPL scores (n=8) after Sportball© participation (∆mean=-0.35 ± 2.52 points, CI 95% [-6.31, 5.60], p=0.89, r=0.05). When scores were adjusted based on age and sex normative data, the physical literacy classifications shifted from beginning and progressing at baseline to progressing and achieving at post-test (Figure 1). Results from the physical competence tasks (n=10) are reported in Table 3. Notably, there was an observed improvement on the CAMSA test with a medium effect, likely attributable to changes in quality of movement skill execution (Table 3). Figure 2 illustrates the change in individual motor skill execution scores between baseline and post-intervention. A per-protocol, sensitivity analysis [19], excluding the participant who attended fewer than 80% of the intervention sessions, found no change in significance for any outcomes. However, a small effect for time spent holding the plank position (n=9; ∆mean=5.27 ± 7.20 seconds; p=0.44; r=0.26) was identified.
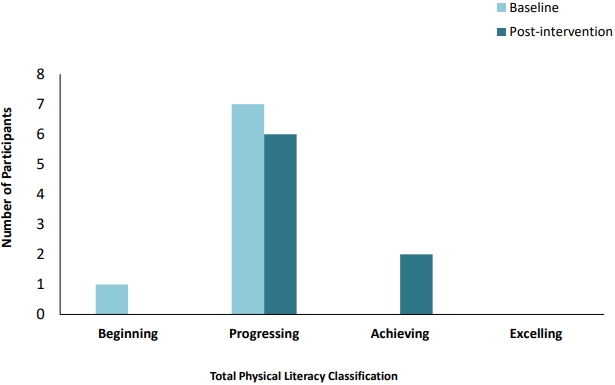
CAPL classifications for total physical literacy at baseline and post-intervention.

Physical competence data
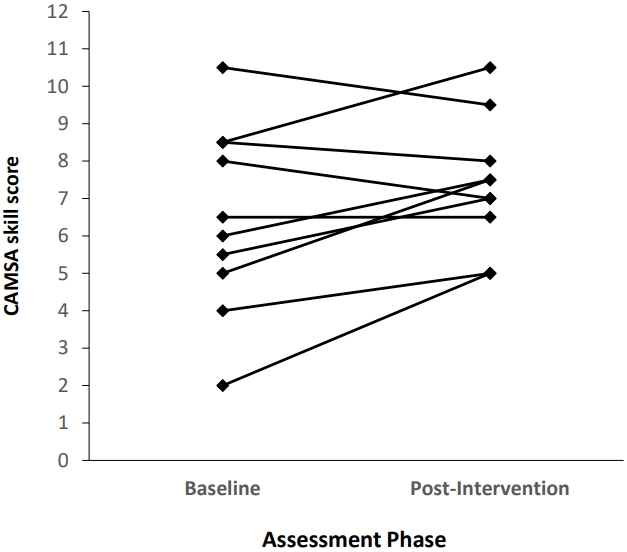
Individual CAMSA score for motor skill execution at baseline and post-intervention
Reflecting on the CAPL during the post-intervention focus group, participants (n=4) indicated a perceived improvement in various tasks. Julia mentioned her performance of the CAMSA, saying: “I’m better now because before, I didn’t really know the obstacle course but now I do know it really well…”. John also perceived an improvement in his torso endurance and strength, when he said that he “especially [improved] with the plank… I broke the record!”; compared to baseline, he spent an additional 27.2 seconds in the plank position at post-test.
Due to device malfunctions (n=1) and poor compliance (n=3), valid accelerometer data were obtained from only 7 participants (64% of total sample; 3 girls, 4 boys). Time spent in moderate-to-vigorous physical activity (Figure 3, F=0.47, p=0.71) and time spent sedentary (F=0.84, p=0.42) did not differ throughout participation. By self-report, the number of days per week spent meeting activity guidelines (i.e., 60 minutes of moderate-to-vigorous physical activity per day) did not differ between baseline and post-intervention (p=0.38; n=8), nor between intervention sessions (p=0.65).
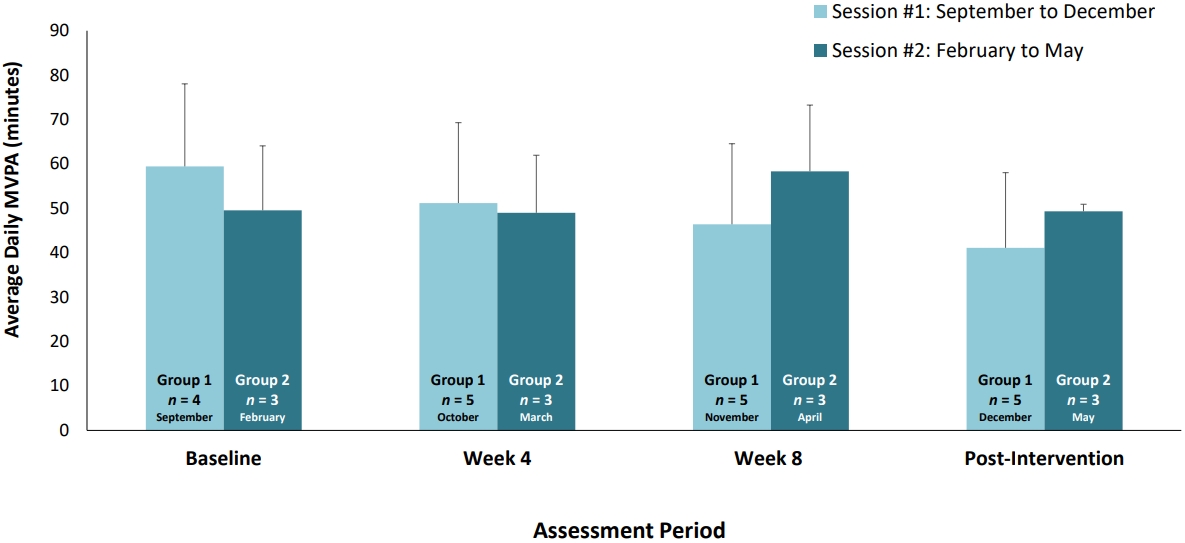
Average time (minutes) recorded by accelerometry in moderate-to-vigorous physical activity per day. Standard deviations from the mean are represented by error bars.
Light green bars = Session #1 (September to December); Dark green bars = Session #2 (February to May)
DISCUSSION
This pilot study evaluated Sportball©, a community-based sport program, and found it to be suitable for children with CHD. Reasons for not participating were primarily logistical (i.e., distance, scheduling conflicts). Further, children with CHD are generally more susceptible to acquiring respiratory illness [23], which was frequently reported as a reason for absence. The capacity of the program to adapt activities by ensuring each child’s needs were met (i.e., accounting for reduced fitness, restrictions, etc.) and providing opportunities for adequate rest contributed to the feasibility of the intervention.
Children with more complex diagnoses of CHD are usually restricted from “competitive sport”, often defined as high intensity, organized sports that test the physical limits of participants [24]. In this study, applicable activity restrictions (73% of participants) were communicated clearly to coaches, which allowed the creation of a safe, yet engaging environment within the constraints of the program. For patients with CHD, restricting sport participation can be a fine line for physicians [7]; distinguishing potentially harmful, strenuous environments from those encouraging recreational play. If this distinction is not communicated clearly, it may result in unnecessary exclusion from sports that indeed are inclusive for children with cardiorespiratory limitations [25]. Alternatively, educating families on the rationale for restrictions may help children with CHD and their parents better understand limitations within sport-based contexts. With this knowledge, children with CHD and their families may be better able to effectively communicate their limitations and subsequent needs to community-based leaders (i.e., coaches, directors), who can accommodate them accordingly.
One salient component informing the feasibility of the program was that all participants were able to determine for themselves when to take necessary breaks. Introducing activity variations allowed participants to more effectively regulate their activity intensity, as children with low exercise capacities could participate without feeling discouraged [26]. Further, once the need for rest was identified by a child with CHD, being in an environment where there was minimal pressure to maintain participation was essential. Therefore, the Sportball© context provided an opportunity for children with CHD to practice self-regulation. Although not implemented into the current intervention, self-regulation techniques may also be helpful tools for children with CHD who need to monitor their activity intensity. For example, the use of the “talk test” (i.e. maintaining conversation while active) is a valid and reliable method for monitoring exercise intensity [27] and has also been recommended for children with CHD [28].
Significant psychomotor/psychosocial deficits, including learning disabilities and ADHD, are common among children with CHD, affecting approximately 30-40% of patients [11]. The design of Sportball©, which emphasizes skill progressions at each child’s pace, allowed the coaches to support all participants, including those with diagnosed deficits. Behaviours demonstrated throughout the intervention (i.e., not wanting to complete skills, hesitation with sport-specific language) may be explained in part, through previous research. For example, children with ADHD have previously demonstrated difficulties applying feedback to movement skills in active contexts [29]. Social deficits among youth with learning disabilities and ADHD are suggested to impact their engagement in physically active contexts (i.e., taking one’s turn, following instructions, etc.) [30]. Therefore, how physical activity programs targeting children with CHD accommodate psychosocial and/or psychomotor deficits is an important factor to consider when evaluating feasibility.
In addition to feasibility, this study provided preliminary results on the benefit of Sportball© for children with CHD, within the context of physical literacy. Our findings support the idea that participation in a recreational sport program may influence components of physical literacy, particularly movement skill and musculoskeletal fitness. The high prevalence of motor skill deficits observed among this population is hypothesized to contribute to their overall sedentary lifestyle by inhibiting participation and reducing self-efficacy for physical activity [13]. Thus, there is practical significance for a child to go from beginning to achieving in motor skill capability, as they may become more likely to engage in regular, active play [31]. Further, perceived improvements in tasks of physical competence were communicated by participants following the intervention. Given the known association between perceived physical competence and physical activity behaviour [32], these self-recognized improvements are important. Knowledge from prior interventions [33-35] suggests that more frequent and/or longer use of the Sportball© program may have led to significant improvements in overall physical literacy outcomes.
As a pilot study, our physical literacy findings are limited by a small sample and single-case design. Given a few instances of non-compliance to study tasks, complete data were not collected from all participants. Finally, while the intervention was feasible, its length (10 one-hour sessions) may not have been sufficient to observe any significant changes in physical literacy. Nonetheless, this study achieved its primary objective of understanding the feasibility of a community-based sport intervention for children with CHD by taking a unique mixed-method approach. Despite the small sub-sample invited to participate in focus groups, important information emerged from the dialogue that complemented objective measures of feasibility and physical literacy outcomes.
CONCLUSIONS
This study provides preliminary evidence to support the feasibility of a community-based sport program for children with CHD, particularly when adaptations accommodate cardiorespiratory limitations, activity restrictions and/or neurodevelopmental delays. The intervention improved participants’ movement skill, from beginning/progressing to progressing/achieving. Along with a trend toward improved torso muscular endurance, these results suggest the need for a controlled trial to examine the impact of Sportball© on physical literacy outcomes among this vulnerable population.
Acknowledgements
We would like to thank participating families and the Children’s Hospital of Eastern Ontario Division of Cardiology for their support of this research. We would also like to recognize Jason D’Rocha, Michael Busse and the senior staff at Sportball© for their support with training and delivery of the intervention. Finally, Jenna Yaraskavitch, Caroline Dutil, Kevin Moncion, Tyler Kung, Anastasia Alpous and Taru Manyanga are all thanked for their assistance with data collection. This work was supported by funding from the Mitacs Accelerate program (grant number IT08244) in partnership with Sportball ©.
Notes
Conflict of Interest
The authors declare no conflict of interest.