



INTRODUCTION
Over the past three decades, increasing attention has been paid to the association between adipose tissue accumulation (particularly intra-abdominal visceral fat) and increased obesity-related morbidity, including those of a young age [1,2]. Several mechanisms for this relationship have been postulated [3]. For example, unlike subcutaneous adipose tissue (SAT), when visceral adipose tissue (VAT) undergoes lipolysis, non-esterified fatty acids are delivered directly into the liver via the portal vein, and if they are in excess, some can accumulate in the liver and lead to insulin resistance and metabolic abnormality [4]. Therefore, it is desirable to minimize the accumulation of VAT from a young age.
Exercise and dietary restriction are both common approaches taken to promote a negative energy balance for people with overweight and obesity. However, to maintain proper development, it is recommended that children and adolescents focus more on increasing physical activity than dietary restriction when treating obesity [5]. In other words, adults are better able to tolerate the reductions in fat-free mass that often occur when trying to lose fat mass [6]. By contrast, children and adolescents should avoid losses in fat-free mass in order to ensure proper development. Therefore, when trying to reduce VAT in children via exercise with or without calorie restriction, it is necessary to set desirable conditions in order to minimize the loss of fat-free mass. Our purpose was to review studies which investigated how exercise training with and without calorie restriction changed VAT/SAT obtained by abdominal imaging and fat-free mass in children and adolescents. This population is of specific interest given that they are still developing and it is important to understand how this may differ with previous work in adults [6].
FINDINGS
Numerous studies investigated the effects of exercise intervention programs with and without calorie restriction on abdominal fatness in children and adolescents [1,7-10]. To achieve the aim of this mini review, a search using the electronic databases (PubMed and Scopus) and a search engine (Google Scholar) was conducted, and intervention trials that reported total body fat, VAT area, and SAT area before and after the intervention were considered eligible for this review. The inclusion criteria were as follows. First, the study needed to include exercise (aerobic and/or resistance) with or without calorie restriction. Second, the study needed to include individuals under the age of 18 with overweight and/or obesity (e.g. body mass index (BMI) >95th percentile). Third, the study needed to measure VAT and SAT areas at baseline and after the intervention. Within the searched articles, there were various methods (i.e. CT, MRI or ultrasound) and protocols (i.e. a single image of the abdomen, multiple images of the trunk, or the whole body) used for evaluating the accumulation of VAT/SAT [2,10]. In the current review paper, we selected those that investigated changes in VAT/SAT using a single abdominal image (VAT and abdominal SAT areas) according to a previous study [2]. Fourth, the study needed to measure total body fat mass (using dual-energy X-ray absorptiometry, densitometry such as underwater weighing or air displacement plethysmography, bioimpedance, and MRI) before and after the intervention. Lastly, the search was limited to original research that was written in English. We found six studies that measured changes following exercise interventions with and without calorie restriction [11-16]. Of these studies, 2 examined the effects of aerobic exercise training alone, 3 examined the effects of resistance exercise training alone, and the other 3 examined aerobic exercise training with calorie restriction (Table 1). Two of the six studies included a control group.
Exercise training without calorie restriction
The findings from studies including aerobic exercise training results in relatively consistent findings with respect to changes in VAT and abdominal SAT areas (Table 2). For example, one study investigated the effects of aerobic exercise training (up to 60 min at 60-75% of individual’s peak oxygen uptake (VO2peak), 3 times per week) on VAT area in girls with obesity. Following 3 months of the intervention, the authors reported significant reductions in VAT area compared with the control group [16]. However, changes were not observed with abdominal SAT area [16]. Similar results were observed following 3 months of aerobic training (30 min at 70% of VO2peak, twice a week) whereby changes in VAT area were noted but abdominal SAT remained unchanged compared to baseline [15]. In contrast, the effects of resistance exercise training on VAT and abdominal SAT areas are different. The three studies observing the effects of resistance training did not show changes in the VAT area compared to a control [12,16] or baseline [13]. Interestingly, two studies found that abdominal SAT significantly increased following resistance training compared to baseline [12,13]. It is not clear why those initiating a resistance training program would increase abdominal SAT. It is possible that this is explained by something other than the initiation of resistance training. Regardless, it is important to examine the relationship between changes in body composition (body fat and fat-free mass) and changes in VAT and abdominal SAT areas.
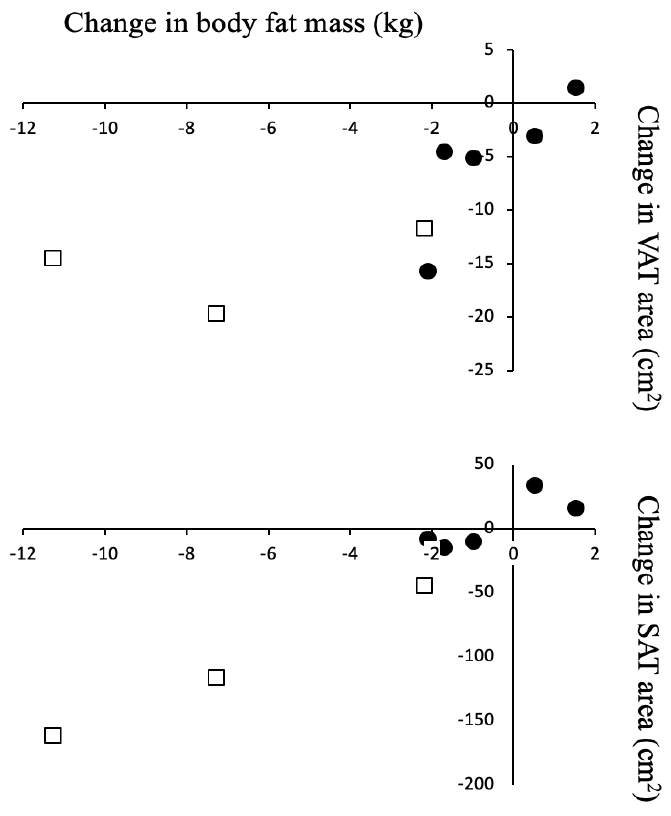
Figure 1 compares changes in body fat mass to changes in VAT and abdominal SAT areas. A previous report found that changes in VAT are primarily determined by changes in fat mass but also the initial VAT to fat mass ratio [17]. In our results, there appeared to be close visual relationship between changes in total body fat and changes in the abdominal SAT area. The relationship between total body fat and changes in VAT area did not appear as clear. These results are consistent with the association with changes in VAT and abdominal SAT areas when adults reduce body fat with a negative energy balance [2]. Interestingly, no reduction in fat-free mass occurred in the exercise interventions without calorie restriction (Table 2). Under these conditions, a decrease in body fat mass will result in a decrease in VAT area.
Exercise training with calorie restriction
The combination of aerobic exercise and calorie restriction increases the loss of VAT area compared with exercise alone but tends to also reduce fat-free mass (Table 2). For example, in one study [11], the inpatient group who underwent calorie restriction and aerobic exercise had a 5.4 kg reduction in fat-free mass. In contrast, the outpatient group with calorie restriction and aerobic exercise lost only 0.5 kg of fat-free mass. This greater loss with the inpatient group might be due to better adherence with the dietary restriction compared to that of the outpatient group. This along with the inpatient group completing more exercise (60 minutes vs. 30 minutes) per day could have increased the energy deficit to a point where fat-free mass would be negatively impacted. Another study, however, found almost no change in fat-free mass following a 3-month intervention [14]. In both of these studies, the degree of calorie restriction was set to 75-80% of individual nutritional requirements. Adding calorie restriction to exercise may help reduce VAT area, but the magnitude of the calorie deficit created may also increase the loss of fat-free mass [18].
CONCLUSIONS
Our review suggests that there are not reductions in fat-free mass in the exercise interventions in which there was no dietary-induced calorie restriction. These results support the idea that reducing visceral fat by increasing physical activity may be preferred over strategies focused on dietary restrictions in children and adolescents. Considering the results of a study implementing strict dietary control [11], it is possible that 75-80% of individual nutritional requirements, when combined with aerobic exercise, could cause a decrease in fat-free mass. Although factors such as the type (e.g. aerobic and/or resistance) of exercise and the amount (i.e. energy expenditure) of exercise will likely have an effect on the magnitude of change in intra-abdominal visceral fat, the quantity of each that is needed in order to reduce visceral fat without reducing fat-free mass is currently unknown. Therefore, future research is required to clarify this topic.