Modification of Cooper’s 12-min Run Test for Valid Prediction of Cardiorespiratory Fitness in Male and Female Boxers of India
Article information

Abstract
OBJECTIVES
This study aimed to evaluate the authenticity for application of Cooper’s 12 min run test (CRT) to predict VO2max in male and female boxers in India.
METHODS
Participants of both sexes (male=70, female=60) were recruited from different boxing clubs in India, and randomly allocated to the study group (male = 40, female = 30) and cross-validation group (male = 30, female = 30). VO2max was directly estimated by bicycle exercise with progressive workload followed by expired gas analysis in a Scholander micro-gas analyzer. CRT method was used for indirect prediction of VO2max.
RESULTS
Predicted VO2max (PVO2max) and directly measured VO2max were found to be significantly (p<0.001) different in the study groups of both sexes, with wide range of limit of agreement between PVO2max and VO2max. This indicates the inapplicability of existing CRT protocol in the male and female boxers. Simple linear regression was computed owing to existence of significant positive correlation (r = 0.84 and 0.89 in males and females, respectively; p<0.001) between VO2max and distance covered in the run test. These newly derived norms depicted insignificant variation between PVO2max and VO2max in the confirmatory group of both sexes.
CONCLUSIONS
Modified equations computed in this study for the prediction of cardiorespiratory fitness in terms of VO2max by CRT were recommended in male and female Indian boxers.
INTRODUCTION
The direct estimation of maximum oxygen uptake (VO2max), which is internationally considered the best indicator of cardiorespiratory fitness, is difficult owing to its complicated and expensive experimental protocol. Direct measurement of VO2max requires well-organized laboratory infrastructure and cannot be performed in field-based studies. Standardized procedures for direct evaluation of VO2max are hazardous and laborious [1]. Therefore, it is desirable to look for simpler procedures to evaluate VO2max especially in field studies where large samples are required in the absence of well-equipped laboratory infrastructure [2].
Applicability of different exercise and non-exercise based indirect methods for predicting VO2max has been validated by proposing modified norms in young Indian university and college students [3,4]. Previous research in female collegiate students in Washington standardized the protocol of 20-meter multi-stage shuttle run test, a globally popular test used in different studies to predict VO2max [5]. Other studies have also standardized the 3 min walking distance in Japanese adults with respect to their age, sex and body composition, and a field-based test that was specifically designed for rowers [6,7]. American College of Sports Medicine (ACSM) conducted a study in moderately well-trained male population belonging to the age group of 18–34 years and proposed a submaximal treadmill running exercise test to predict VO2max [8].
Studies pertaining to the indirect prediction of VO2max commonly recommends that the protocol should use as few inexpensive instruments as possible following the appropriate population–specific validation of the protocol [9].
Among the various protocols for VO2max prediction, Cooper’s 12-minute run test (CRT) is a popular one. This requires only a measuring tape to measure the distance covered in 12 min. This test was standardized and recommended in Western populations [10]. Hence, the test must be validated before it can be applied in other populations.
Authentic validation of several indirect protocols for prediction of VO2max including that of the CRT has been performed in non-athlete populations of India [11,12]. However, identical investigations on Indian sportspeople are unavailable. Separate valid protocols are required for sedentary populations and athletic counterparts from different backgrounds because the latter groups undergo various physiological adaptations following participation in sports–specific training programs.
Boxing involves high-intensity intermittent bursts of activity that require anaerobic and aerobic source of energy to sustain the high energy demand of the game. Boxers must sustain power at a high percentage of VO2max [13]. Lithuanian national-level boxers in different weight categories exhibited a significant correlation between VO2max and ranking. This study proposes that special attention should be paid to the development of cardiac capacity in boxers to optimize their performance [14]. Hence, developing optimum cardiorespiratory fitness (VO2max) among boxers is a major concern for trainers and athletes, and frequent intermittent evaluation of VO2max during the training regimen is essential. However, the applicability of indirect protocols for VO2max estimation in boxers has not been reported.
Therefore, this study was conducted to enumerate the accuracy of CRT in predicting VO2max in male and female Indian Boxers.
METHODS
Study population
Boxers (male = 70, female = 60) with at least five years of training background and belonging to 20–25 years of age were randomly recruited in the present investigation from different boxing clubs in Kolkata, India. Sample size was calculated by using PS-Power and Sample Size Calculation software version 3.0.43 (Vanderbilt University, USA) [15]. The recruited participants were randomly divided into a study group (male = 40, female = 30) and a confirmatory group (male = 30, female = 30). The existing CRT protocol, as proposed by Cooper [16], was tested in the study group, and necessary modifications were made to fit the current study population. The modified protocol was tested among boxers belonging to the confirmatory group to assess the validity of the modified norms.
The participants were free from any medication and had no history of any chief medical complaints. They reported to the laboratory in the morning after taking the breakfast 2–3 hours prior to the test. The experimental procedure was elaborated to them to dispel their worry. Participants avoided physical activity on the day of the experiment.
The study was conducted under an ambient temperature ranging between 28 and 32°C. Relative humidity varied between 64 to 75% during the time frame of October 2018 to February 2020. Institutional Human Ethics Committee provided the ethical clearance to conduct the study (IRB No. IHEC/AB/P75/2018 dated 03.07.2018). All the participants provided written informed consent.
Experimental design
Both direct and indirect CRT methods were used to evaluate the maximum oxygen consumption in each participant. A gap of at least 4 days was maintained between the tests [1,2]. A Polar heart rate monitor was used to record the pre-exercise and working heart rates [9,10]. Before exercising, participants rested in a supine position for 30 min to allow the cardiopulmonary parameters to settle to a steady state [1,2].
Prediction of maximum oxygen uptake capacity (PVO2max) by CRT method
The procedure proposed by Cooper [16] was implemented for prediction of maximum oxygen uptake by allowing the participants to run for 12 min at the maximum possible pace on a 400-meter round track. Maximum effort of the participants was ensured by motivating them with verbal encouragement. The total distance (in meters) covered by the participants during this 12 min run was calculated by multiplying the number of laps by 400 and adding the distance if there was any incomplete lap at the end of the run. The distance (in meters) ran over in 12 min was converted into kilometers, and VO2max was predicted by using the following equation [16]:
VO2max(ml·kg–1·min–1) = (22.351 × Distance covered in kilometers) – 11.288
Direct measurement of maximum oxygen uptake capacity (VO2max)
Direct measurement of VO2max in male and female participants was performed using a standard exercise protocol with Müller’s magnetic brake bicycle ergometer (Max Plank Institute of Ergology, Germany) [1,2].
Participant was considered exhausted according to standard guidelines [1,2]. Douglas bag was used to collect samples of expired gas at the last minute of the exercise trial. Aliquots of expired air were analyzed in a Scholander micro-gas analyzer using the procedure of Consolazio et al. [17].
Statistical analysis
Data are presented as mean ± standard deviation (SD). Paired t-tests were performed to determine whether there were any significant differences between the mean values. Pearson’s product–moment correlation coefficient was computed to test for any significant correlation between VO2max and the distance covered in the CRT as dependent and independent parameters, respectively. Linear regression statistics were used to compute the population–specific regression norms. Limit of agreement analysis [18] was executed to confirm the appropriateness of the indirect CRT protocol in the studied population. SPSS version 20 was used for statistical analysis, and all statistical significance levels were set at p<0.05.
RESULTS
Distance covered in CRT and physical as well as physiological parameters are presented in Table 1. Age did not show any inter–sexual variation. However, distance covered in CRT, body height, weight and blood pressure were significantly (p<0.001) different between the male and female boxers.

Physical and physiological parameters and distance covered in CRT of the male and female boxers.
The results of the Bland–Altman method of the limit of agreement analysis in both the study groups are shown in Figure 1 and 2, respectively. Significant difference between VO2max (49.31±5.59 ml·kg-1 ·min-1 in males and 45.52±4.12 in females) and PVO2max (59.64±3.94 ml·kg-1·min-1 in males and 54.88±4.23 ml·kg-1 ·min-1 in females) was observed in the study group of both sexes. The Bland-Altman [12] limit of agreement analysis method depicted a wide range of variation between PVO2max and VO2max (1.34 to 19.38 ml·kg-1·min-1 in males and 5.52 to 13.2 ml·kg-1·min-1 in females) with poor confidence intervals in both the sexes (Figure 1 and 2). This specifically signifies that the existing norm of CRT, as proposed by Cooper [16] is not applicable to the studied population for the valid prediction of VO2max.
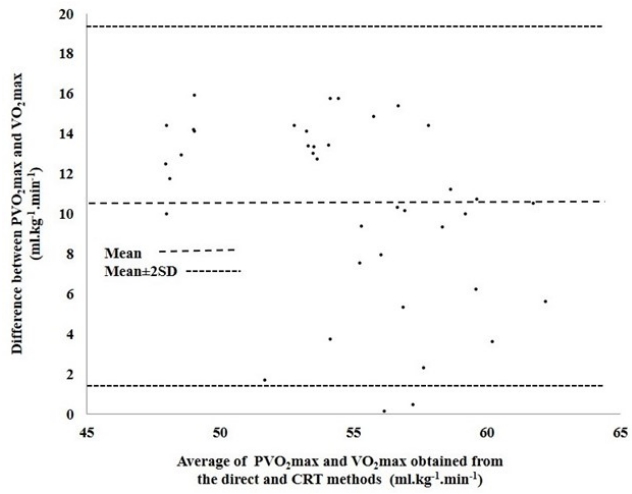
Plotting of differences between the predicted values of maximum oxygen uptake capacity (PVO2max) and directly measured values of maximum oxygen uptake capacity (VO2max) against the average of directly and indirectly measured values of maximum oxygen uptake capacity in the study group of male boxers.
Abbreviations: SD, standard deviation; CRT, Cooper’s 12 min run test.
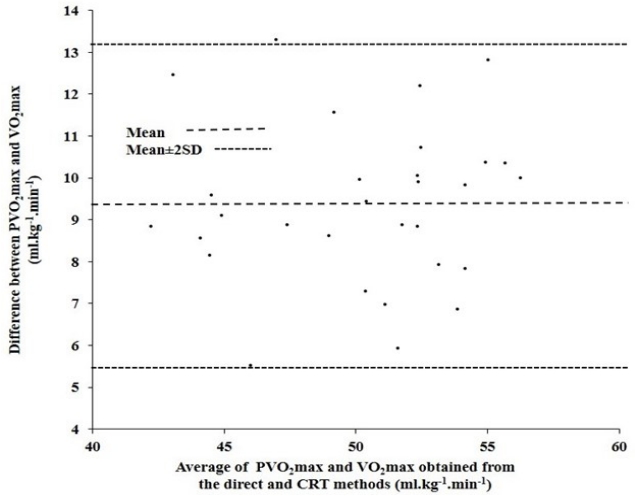
Plotting the difference between predicted values of maximum oxygen uptake capacity (PVO2max) and directly measured values of maximum oxygen uptake capacity (VO2max) against the average of directly and indirectly measured values of maximum oxygen uptake capacity in the study group of female boxers.
Abbreviations: SD, standard deviation; CRT, Cooper’s 12 min run test.
The results of the correlation analyses and regression norms for male and female boxers are plotted in Figure 3 and 4, respectively. Significant correlation was observed between distance covered in CRT and directly estimated VO2max in both the study groups (r = 0.84 in males and r = 0.89 in females, p<0.001). Regression equations were computed in male [Y = 13.92 X + 2.94 (SEE = 3.04 ml·kg-1·min-1)] and female [Y = 19.48 X – 12.15 (SEE = 1.87 ml·kg-1·min-1)] study groups for reliable prediction of VO2max in the studied population (Figure 3 and 4).
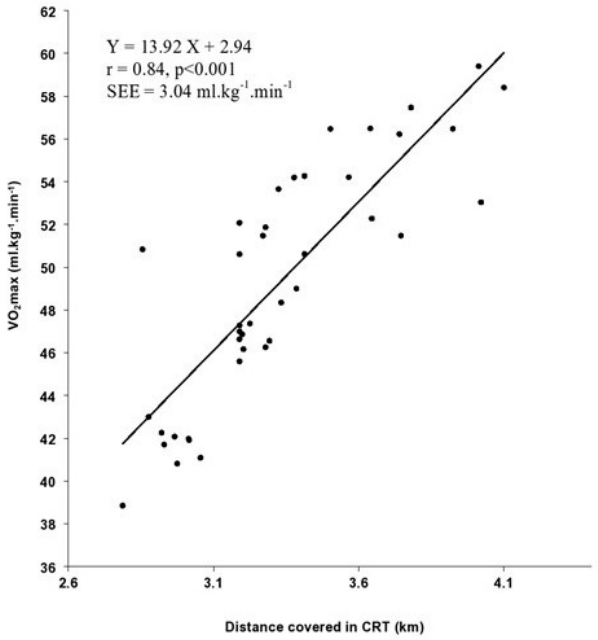
Relationship between maximum oxygen uptake capacity (VO2max) and distance covered in Cooper’s 12 min run test in the study group of male boxers.
Abbreviation: CRT, Cooper’s 12 min run test.
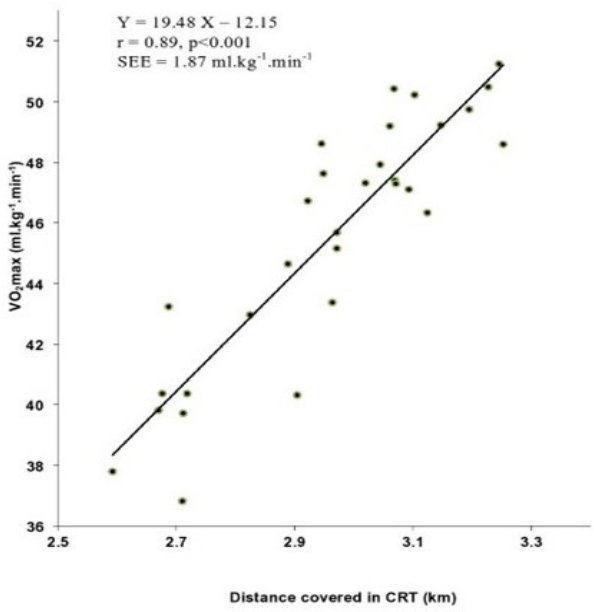
Relationship between maximum oxygen uptake capacity (VO2max) and distance covered in Cooper’s 12 min run test in the study group of female boxers.
Abbreviation: CRT, Cooper’s 12 min run test.
The applicability of these newly derived equations was tested on the respective confirmatory groups, revealing an insignificant difference between PVO2max, determined using the modified equations (47.19±4.07 ml·kg-1·min-1 in males and 46.17±3.72 ml·kg-1·min-1 in females) and directly measured VO2max (48.16±4.12 ml·kg-1·min-1 in males and 45.16±3.19 ml·kg-1·min-1 in females).
Further analysis of data obtained in the confirmatory group of both the sexes, applying the Bland–Altman analysis and repeatability test, indicated a narrow range of difference between VO2max and PVO2max. These values were insignificantly different from zero and fell within the ±2SDs.
DISCUSSION
The determination of VO2max is essential during different phases of training because it is one of the key factors indicating an athlete’s response to a training protocol and their potential for improvement in performance capability. Boxers must delay the onset of fatigue with increased tolerance to lactic acid production to sustain a high-power output at a high percentage of VO2max [13]. Hence, the objective of the present investigation will not only serve to monitor the overall health of boxers, but also serve as an easy tool to intermittently evaluate the effect of training on cardiorespiratory fitness.
The VO2max values of female boxers are consistent with those reported in a previous study [19]. In contrast, the VO2max value of male boxers was lower than that of their national-level North Indian counterparts [13]. The VO2max value in elite male Indian Boxers (54.5 ml·kg–1·min–1) was higher than the value observed in the present research [20]. The applicability of the presently modified equations will be restricted to Indian Boxers aged 20–25 years, since it has also been reported that VO2max values differ significantly among different age groups [13].
The indirect prediction of VO2max from the modified equations showed less than 5% variation in 52 male and 45 female subjects, 5–9% variation in eight male and seven female subjects, 10–14% variation in six male and four female subjects, and 5–19% variation in four male and four female subjects from their corresponding respective directly measured value of VO2max.
The VO2max values thus predicted and directly measured in the confirmatory group were analyzed by limit of agreement analysis of Bland and Altman, which indicated considerably narrow range of limits of agreement in the male (–0.324 to 2.354 ml·kg–1·min–1) and female (–0.234 to 2.286 ml·kg–1·min–1) boxer groups of the present study. The percentage of variation between VO2max and PVO2max decreased from 20.94% to 3.67% in male boxers and from 12.1% to 2.08% in female boxers following the application of the revised population-specific equations.
Repeatability tests were conducted according to the Bland-Altman method [18] to further confirm the validity of the modified equations for the studied population. Repeatability coefficient is defined as the 95% confidence interval for measured parameters that lie within two SDs (±2SDs) [21]. This criterion was met in the present study, where the values of PVO2max and VO2max were not significantly different from zero and were within the ±2SDs in both the sexes.
The equations developed in this study are applicable only to male and female boxers in India belonging to the studied age group. This is a major limitation of the study that these equations cannot be applied to other categories of sportspersons or sedentary populations.
CONCLUSIONS
The present study indicates that the original CRT protocol, as proposed by Cooper [16], cannot be used to predict VO2max in male and female boxers. However, the modified equations proposed in the present study predicted the VO2max quite precisely in the studied population. These newly derived norms are therefore recommended for the application of Cooper’s 12 min run test for the valid and accurate prediction of cardiorespiratory fitness in terms of VO2max in male and female boxers of India.
Acknowledgements
The author is indebted to the participants for their whole–hearted support to complete the study.
Notes
Conflicts of interest
The author declares no conflicts of interest.