Effects of Yoga on Measures of Health-related Quality of Life from SF-36 and SF-12 Assessments: A Systematic Review and Meta-analysis
Article information
Abstract
Objectives
Yoga is commonly being adopted and prescribed with the intent to increase a participant’s health-related quality of life. In practice, the current gold-standard health-related quality of life measurement tool is the SF-36 and SF-12 assessments. Therefore, it is important for yoga scientists and practitioners to understand yoga’s effects on health-related quality of life when in fact a gold-standard assessment is implemented. The purpose of this study was to employ systematic review and meta-analytic techniques to examine the effect of yoga on measures of health-related quality of life measured using only the SF-36/12 assessments.
Methods
A current (January 2007 to December 2016) systematic review of the Pubmed database was conducted and included studies that used yoga as an intervention with outcomes measures of health-related quality of life measured by the SF-36/12. Ten different measures were extracted from studies including eight dimension scores (physical functioning, bodily pain, physical role function, general health, mental health, emotional role function, social function, and vitality) and two summary scores (physical component and mental component). Ten different meta-analyses were performed using calculated standardized mean effect sizes and random effects models. Both moderator and sensitivity analyses were conducted.
Results
A total of 34 studies were included is the analyses with 185 independent effect sizes. Yoga intervention showed a significant positive effect on all ten measures of the SF-36/12. Effects ranged from 0.56 (0.39-0.73) to 0.28 (0.17-0.40). Yoga type (Hatha, Iyengar, Other) moderated the effects of yoga intervention on the mental component (p=.021), with Hatha yielding the greatest effects (ES=1.63, 0.61-2.65). The sensitivity analysis showed little to no bias in mean effect size estimates.
Conclusions
The meta-analytic evidence clearly supports the small-to-medium positive effects of yoga on health-related quality of life, as measured by the SF-36/12 assessments.
INTRODUCTION
The Hindu philosophy of yoga, originating during the second century B.C, is based on eight limbs of Ashtang yoga: 1) compromised of ethical disciplines, 2) individual observances, 3) posture, 4) breath control, 5) withdrawal of senses, 6) concentration, 7) meditation, and 8) enlightenment [1]. In western societies, the term yoga is now a general term that describes a practice which focuses on breathing techniques, postures, strengthening exercises, and meditation [2]. Many forms of yoga exist with some of the more popular being Hatha, Iyengar, and Vinyasa which all aim to promote physical and psychosocial conditioning with improved wellness [3]. Yoga has increasingly become popular as a form of medicine to treat and prevent certain diseases [4,5,6]. A review of several meta-analyses showed that yoga has a positive effect on physical fitness, metabolic function, and other physical health related outcomes [7]. In terms of mental health, yoga has shown to be an effective treatment for those suffering from clinically diagnosed major depression [8,9]. Studies have also shown that yoga can improve both physical and mental health in a variety of generally healthy yet diverse populations [10,11,12].
Another outcome measure of growing interest in medical research is health-related quality of life (HRQOL). HRQOL is defined as a multi-dimensional concept that includes domains related to physical, mental, emotional, and social functioning. It goes beyond direct measures of population health, life expectancy, and causes of death, and focuses on the impact health status has on quality of life [13]. HRQOL has become a routine measure for clinicians to use in order to evaluate the effects of a chronic disease or illness on their patients [14]. Similar to other outcome measures, yoga has also shown to improve measures of HRQOL. Several studies have shown yoga improves HRQOL in individuals with cancer, arthritis, and chronic bodily pain [15,16,17].
There are several HRQOL measurement tools that have been developed and used in physical activity-related research [18]. However, the more widely used assessment tool is the Medical Outcomes Study 36-Item Short Form Survey (SF-36). The SF-36 is a multipurpose health survey that consists of 36 questions and yields an eight-scale profile of scores as well as a physical and mental health summary measure [19]. The SF-36 is such a widely-used instrument because it was designed as a generic instrument that would be applicable to a wide range of types and severities of health conditions [20]. The SF-12 is a condensed version of the SF-36 which consists of only 12 questions and has demonstrated to be equally reliable and valid as the SF-36 in clinical and population based studies in the US and other countries [21].
The SF-36/12 uses multi-item scales to measure the following 8 dimensions that cover the major concepts of ones HRQOL [20]:
• PF- Physical Functioning
• BP-Bodily Pain
• PRF-Physical Role Functioning (Role limitations due to physical health problems)
• GH-General Health Perceptions
• MH-General Mental Health
• VT-Vitality, Energy, Fatigue
• SF-Social Functioning
• ERF- Emotional Role Functioning (Role limitations due to emotional problems)
There are two sets of scores that are derived from administration of the SF-36/12: a profile score for the 8 dimensions and two summary scores, one for the physical component (PCS) and the mental component (MCS) [19] The PCS summary score is made up of scores from the physical functioning (PF), bodily pain (BP), physical role function (PRF), and general health (GH) dimensions. The MCS summary score is made up of scores from the mental health (MH), emotional role function (ERF), social function (SF), and vitality (VT) dimensions [20].
Many meta-analysis have shown the potential benefits of yoga on measures of HRQOL in numerous clinical populations [22,23,24]. However, although there has been research done on the effects of yoga on measures of HRQOL, none to date have measured the overall effect size of yoga on HRQOL measured by the SF-36/12. Therefore, the purpose of this meta-analysis was to explore and analyze the effect of yoga on measures of HRQOL measured using only the SF-36 or SF-12.
METHODS
Literature Search
Two reviewers conducted a search in PubMed database for studies that were conducted using yoga as an intervention and HRQOL measured by the SF-36/12 as an outcome measure. The following keywords were used to conduct the search in PubMed: yoga (“health-related quality of life” or “sf-12” or “sf-36” or “sf-8” or PCS or MCS or HRQOL or “mental component” or “physical component”).
Inclusion and Exclusion Criteria
Following a search using the above keywords in PubMed, two reviewers independently analyzed the abstracts generated using the following inclusion criteria:
1. Publication type: Included studies had to have been published in a peer-reviewed journal indexed in Pubmed.
2. Date of study publication: Included studies had to have been published within the past 10 years. The search began in September of 2016 and continued till December of 2016 with the cutoff date of 2007.
3. Type of design: Included studies had to be experimental in design and be either a randomized controlled trial or single group with pre- and post-intervention measurements.
4. Types of Intervention: Interventions had to use yoga as the main exposure. Studies that used yoga with a combination of other exposures where yoga was not a dominant exposure were not included.
5. HRQOL measure: Only yoga interventions that used the SF-36 or SF-12 were included.
If all inclusion criteria were met for a study based on review of its abstract, a full text of the study was retrieved for further evaluation. As well, if inclusion criteria were not able to be evaluated based on information given in an abstract, a full text of the study was retrieved. A second stage of independent reviews was then performed with all full-text articles by the same two reviewers. Studies were excluded at this point of the systematic review if 1) any of the inclusion criteria above were in fact not met or 2) it was apparent that the type of data analysis performed in the study was not conducive to a standardized mean difference meta-analysis.
Data Extraction
Data for each study was independently extracted by the two reviewers using the same spreadsheet template to assure consistency. The following data were extracted from each of the included studies: Last name of the first author, publication year, type of study design, SF-36/12 form used, SF-36/12 measures reported, intervention sample size, intervention mean age, gender of sample, duration of yoga intervention (months), days per week of yoga intervention, and the form of yoga. Depending on study specifics, the following additional data were extracted: pretest, posttest, or gain score means and standard deviations; test statistics; confidence intervals; or p-values. After all data were extracted, both data-sets were compared for uniformity. After both datasets were consistent, one final dataset was created to be used for the final analysis.
Statistical Analysis
Ten different meta-analyses were performed in total including one for each of the eight SF-36/12 dimensions and one for each of the SF-36/12 summary component scores. Each meta-analysis was performed using calculated standardized mean effect sizes and their standard errors [25]. Due to the large scope of studies included in the systematic review, studies representing different randomly drawn populations from a universe, it was assumed that true differences existed across effect sizes. In other words, it was assumed that different populations (e.g., diseased vs. non-diseased) experienced different effects due to yoga intervention. Therefore, random effects models were used for all analyses [26]. Forest plots were constructed to describe individual study-level effect sizes as well as each pooled effect size with 95% confidence interval (CI) [27]. To further describe variability in effect sizes, the Q statistic for heterogeneity, the tau-squared (τ2) representing the variance component, and I2 describing percent of heterogeneity were computed [28].
A moderator analysis was conducted for each meta-analysis and included the categorical factors of study design, gender, disease status, yoga type, and SF-36/12 form. Two continuous variables were also used in the moderator analyses and included intervention length and participant mean age. All moderator analyses were performed using random effects models with non-pooled variances (τ2) [29]. A Q statistic provided statistical evidence against homogeneity of effect sizes for each moderator analysis. Finally, a three-step sensitivity analysis was performed for each meta-analysis. First, Egger’s regression models were used for testing funnel plot asymmetry [30]. Second, a trim-and-fill method was used for estimating the number of effect sizes required to show a symmetric funnel plot [31]. This method also provided an estimated mean effect size with the imputed study effect sizes required to balance the funnel plots. And lastly, a leave-one-out analysis was performed by re-estimating the effect sizes once for each study deleted [32]. Both Comprehensive Meta-Analysis (CMA) and the R Metafor package were used for the analyses [33,34]. Significance was set to p<.05. Standardized mean difference effect size (ES) thresholds were set as follows: .20 (small), .50 (medium), .80 (large) [35].
RESULTS
The initial search found 114 abstracts with 54 identified for full-text retrieval. From the pool of full-text studies, after further review, an additional 20 studies were excluded. This resulted in 34 studies being included in the meta-analysis with 185 independent effect sizes. The number of effect sizes ranged from 16 to 24 across the ten SF-36/12 measures. Figure 1 summarizes the search strategy with inclusion and exclusion reasoning. Table 1 describes the 34 studies in terms of their characteristics [36-69].
Schematic depiction of search strategy.

Characteristics of included studies
Figure 2 contains study-level mean effect sizes with 95% CIs as well as the pooled mean effect size and 95% CI from the random effects model. Yoga intervention showed a significant positive effect on the SF-36/12 MCS (ES=0.56, 0.39-0.73). Figure 3 contains additional forest plot data for the four SF-36/12 mental health dimensions. Each of the four mental health dimensions were significantly affected by yoga intervention, with the smallest effect seen on ERF (ES=0.30, 0.14-0.46) and the largest effect seen on VT (ES=0.47, 0.22-0.73).
Forest plot of MCS effect sizes and random effects (RE) pooled estimate.
Forest plots of effect sizes and random effects (RE) pooled estimates across mental health dimensions.
Figures 4 and 5 show similar random effects forest plot results for physical health measures. The pooled mean effect for yoga intervention on the SF-36/12 PCS was significant (ES=0.28, 0.13-0.44), although lower than that seen for the MCS. As well, all four physical health dimensions saw significant effects from yoga intervention, with the smallest effect seen on GH (ES=0.28, 0.17-0.40) and the largest effect seen on BP (ES=0.41, 0.23-0.58).
Forest plot of PCS effect sizes and random effects (RE) pooled estimate.estimates across mental health dimensions.
Forest plots of effect sizes and random effects (RE) pooled estimates across physical health dimensions.
Table 2 contains additional statistical support for heterogeneity of effect sizes across the ten SF-36/12 measures. All Q statistics, testing against homogeneity, were significant (ps<.05). As well, I2 values were considerable with the smallest I2 seen for PF (35.4%) and the largest seen for VT (90.4%).

Summary results and variance components across SF-36/12 component scores and dimensions.
Table 3 displays results of the random effects moderator analysis on the MCS and mental health dimensions. Only a few factors showed significant Q statistics, indicating moderating effects. Namely, yoga type moderated the effect of yoga intervention on the MCS (p=.021), with Hatha yielding the greatest effects (ES=1.63, 0.61-2.65). As well, SF-36/12 form showed a significant moderating effect on VT (p=.026), with the SF-36 producing a significant effect (ES=0.50, 0.23-0.77) and the SF-12 producing no effect (ES=0.03, -0.29-0.35). For the continuous moderator analysis, length of yoga intervention significantly moderated MH (ES=0.03, 0.01-0.06) and VT (ES=0.06, 0.03-0.10) dimensions.

Effect size by moderator for the SF-36/12 MCS and mental health dimensions.
Table 4 displays similar random effects moderator analyses for the PCS and physical health dimensions. Only two factors showed significant Q statistics, both on the PRF dimension. Namely, for the gender analysis, studies with both sexes showed that yoga intervention significantly (p=.004) affected PRF (ES=0.37, 0.22-0.52) and had no effect in studies with females only (ES=0.00, -0.20-0.20). As well, SF-36/12 form showed a significant moderating effect on PRF (p=.028), with the SF-36 producing a relatively smaller effect (ES=0.28, 0.13-0.44) as compared to the SF-12 (ES=0.69, 0.36-1.01).
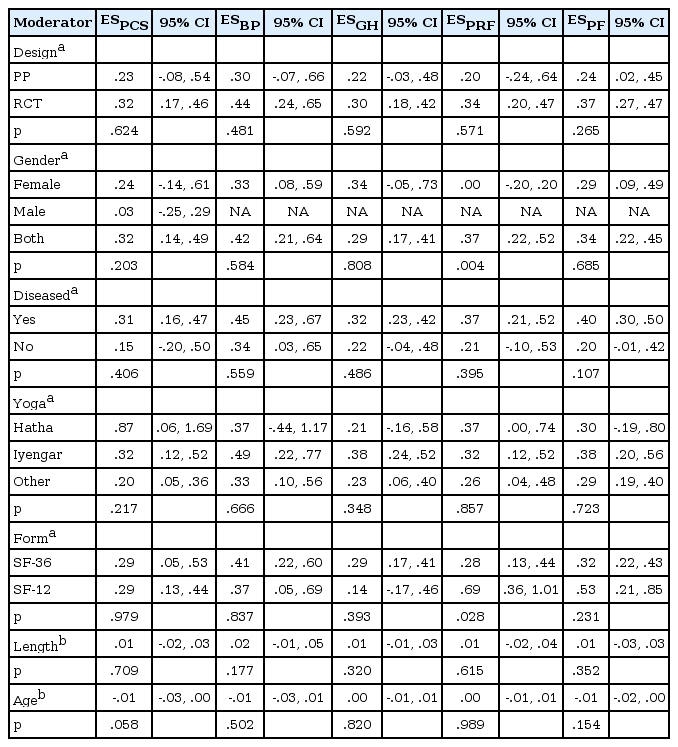
Effect size by moderator for the SF-36/12 PCS and physical health dimensions.
The sensitivity analysis, in whole, showed little to no bias in mean effect size estimates. Egger’s regression test for funnel plot asymmetry showed only one significant Z statistic (p<.001), which was for the MCS. However, the trim-and-fill analysis for the MCS, after imputing four effect sizes, re-estimated an effect that remained significant (ES=0.44, 0.24-0.63). The leave-one-out analysis, as well, indicated robust findings. All lower-bound effect sizes remained significant, with the lowest lower-bound effect seen for the ERF dimension (ES=0.25, 0.11-0.39).
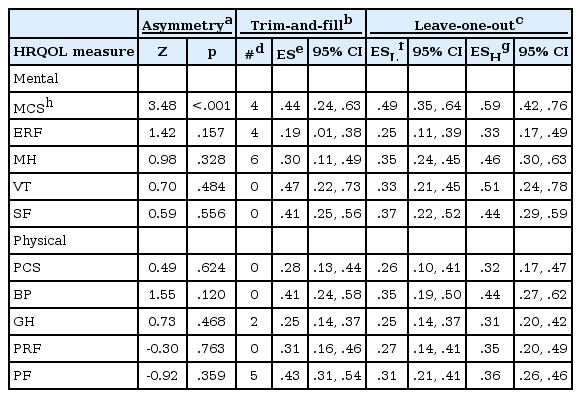
Sensitivity analysis of effect sizes across SF-36/12 component scores and dimensions.
DISCUSSION
The purpose of this research was to perform a systematic review and meta-analysis of published studies from peer-reviewed journals that examined the effects of yoga intervention on measures of HRQOL assessed by the gold-standard SF-36/12 instruments. The primary aim was to evaluate the extent to which yoga intervention affects SF-36/12 measures. Results clearly showed that yoga has a positive effect on HRQOL as measured by the SF-36/12. These results were consistent across both mental and physical health domains. Using the previously mentioned strength effect size thresholds of .2 for small, .5 for medium, and .8 for large, results here support small- to medium-sized HRQOL effects from yoga. These effects remained robust after controlling for both selection bias and any specific study’s influence on the meta-analyses.
Results of this research are also consistent with other meta-analyses examining yoga’s effect on HRQOL. One such meta-analysis indicated that yoga improved psychological health in cancer patients more so than control [22]. However, that analysis was limited to a single measure of HRQOL as well as limited to a specific study population. Another meta-analysis, examining yoga’s effect on the two SF-36 component scores, showed positive effects in favor of yoga for both measures [70]. However, that systematic review was limited to studies published no later than 2010 and was also limited to the two component scores only. A final, and more recent meta-analysis, examined yoga’s pooled effects on HRQOL among women with breast cancer [24]. Although an overall yoga and HRQOL effect was noted in this study, final results were mixed due to positive effects seen by the control over yoga on physical health.
The secondary aim of this study was to determine the extent to which study-level factors and covariates explained heterogeneity across yoga intervention effect sizes. Despite clear heterogeneity, as shown by significant tests of homogeneity (Q statistics), these results were unable to explain such variance. This may be due in part to the imprecise nature of study-level data extracted from articles over that of more precise individual-level data.
This research has limitations that should be considered along with its implications. First, and primary, is the inability of the researchers in all included studies to “blind” yoga participants to their intervention treatment. With yoga intervention participants aware of their treatment, there is no way to remove subject-expectations as a potential threat to internal validity [71]. That is, there is no way to rule out the possibility that yoga participants responded more favorably to follow-up SF-36/12 assessments merely because they knew they were receiving yoga treatment. Second, there were no unpublished or non-peer-reviewed studies included in this systematic review. Excluding these studies are thought to lead to publication bias and in turn cause asymmetric funnel plots [72]. Publication bias was, however, not found to be an issue in this meta-analysis. Moreover, studies that are unpublished are more likely to be of low methodological quality and therefore less useful in terms of unbiased generalizations [73]. A last limitation of this research was the imprecise measurement of yoga treatment. At best, studies included in this meta-analysis reported yoga intervention type (e.g., Hatha), duration (i.e., 30 minutes) and length (i.e., 4 weeks). This type of intervention reporting does not allow for a precise yoga dose measurement. It is of standard practice that physical activity interventions use stringent measurement protocols so as to properly evaluate the effects due to specific doses of activity [74].
There are many strengths, however, associated with this research that are worth mentioning. First, to date, there are no PubMed published studies that have meta-analyzed the effects of yoga intervention on HRQOL specifically assessed by the SF-36/12 set of instruments. This feature adds strength to this research because the SF-36/12 tools are widely known, extensively used, and possess strong psychometric properties [75]. Results from this meta-analysis, showing clear evidence in support of yoga’s positive effect on HRQOL, therefore, have the added value of strong internal validity due to the use of a gold-standard assessment. A second strength of this study is that it included the analysis of ten (10) different HRQOL measures, representing both mental and physical health domains. Since all ten (10) measures showed positive mean effect sizes, results from this meta-analysis have the added assurance of robust generalizations.
CONCLUSIONS
In conclusion, this study performed a systematic review that resulted in the meta-analysis of 185 effect sizes, extracted from 34 published studies, representing ten (10) different SF-36/12 measures of HRQOL. The meta-analytic evidence clearly supports the small-to-medium positive effects of yoga on HRQOL. These effects remained consistent after controlling for various forms of bias. It is suggested that yoga interventions include more precise yoga dosage measurement, as this may in part explain differences in the effects seen.
Notes
Conflicts of interest
The authors declare no conflicts of interest.